I recently had a patient visit me for hormonal consultation. For her chief complaint, she listed “my hormones are going crazy.” After some discussion, she revealed that that her hormones were “out of control all the time,” and that they were affecting her quality of life. She stated she had recently been to another provider who told her that “there is no way your hormones could be causing these things – you probably should see a psychiatrist.” Obviously, she did not feel that that advice was very helpful, and after doing some research she had come to the conclusion on her own that, yes, her hormones were causing symptoms.
Our visit was relatively uneventful – she complained of very common symptoms, such as fatigue, weight gain, low sex drive, and an overall sense of “meh.” We talked about potential causes for her symptoms, and I did a physical exam to rule out any obvious anatomic issues (enlarged thyroid, nipple discharge, etc.). We also talked about labs – when, and if, we should order them, and what they might show. In the end, we ended up drawing a fairly standard assortment of laboratory tests, including a blood count, chemistry panel, thyroid profile, and sex hormones. I had her make a return appointment to discuss results, as well as a plan of care.
A few days later we sat in my office, and went over the results. Her complete blood count -totally fine. Comprehensive metabolic panel – no issue. Thyroid panel – negative. Sex hormones – age and cycle appropriate. “How can this be?” She asked. She had the symptoms of a hormonal issue, but the labs provided no answer to her questions. Unfortunately, this is an all too common finding. Even if we look at the labs with a narrower range of “normal,” there are still many times that they do not provide any answer to why someone feels the way they do. In my opinion, this is one reason why we should treat people, and not lab findings, but that’s another blog. That said, it does no good to put someone on, for instance, testosterone replacement if they do not have a testosterone deficiency, so you can’t just treat symptoms without cause.
So now the question becomes “what do we do?” More often than not, the hormonal symptoms that people complain of are not due to some innate, organic dysfunction, but rather a mix of different factors: sleep, stress, diet, etc. Obviously, symptoms require investigation, and it’s the hope of patients and practitioners everywhere that those investigations yield a diagnosis (one that’s treatable, preferably). But more often than not, unfortunately, those queries seem to only yield more questions, such as what to do with labs that are all within normal range, imaging studies that are unremarkable, and so on.
We are left many times without definitive answers in medicine – although we often wish this wasn’t the case. Just as human beings are full color, three-dimensional, complex beings, so too are the things that ail us; disease processes are not simply black and white. When modern medicine fails to give us answers, many of us are left feeling lost. Now, some may turn into alternative, complementary health care practices – clinical nutrition, herbalism, reiki, etc., while others may research even more occult diagnoses, convinced that they are afflicted with conditions that have only affected a small number people. Neither decision would be an incorrect approach – when we’re feeling bad, we often search for answers in a variety of places. I would caution, however, against therapies or treatments that may seem too good to be true. I have seen many ads on the Internet for supplements that “cure all sexual issues,” or for “specialty clinics” that have a 100% success rate in treating symptoms using a proprietary blend of various therapies. Along the same vein, extremely rare medical conditions do exist, but it can be an expensive and frustrating endeavor to rule out every condition that has a symptom of, let’s say, fatigue.
As for our patient from above, in the end we did find a diagnosis, although not one that was necessarily “hormonal.” Further discussion of her sleep habits revealed that she was getting only a few hours of uninterrupted sleep at night. Her husband also divulged that she snored quite a bit, and would also “startle” while she was asleep. A sleep study confirmed the diagnosis of sleep apnea, and I can say that at her last follow-up, she is feeling 100% better thanks to her CPAP.
The take-home message is this. Hormonal symptoms may be from hormonal causes. They may also, however, be from a variety of nonhormonal factors such as sleep deprivation or stress. In the end it behooves the practitioner to look at the patient as a whole, and not just as an organ system or specific symptom. As I’ve said before, people are more than just a collection of vital signs, lab studies, and complaints. A very good friend of mine (who is a family physician) once told me that western medicine is “really good at treating disease, but terrible at treating symptoms.” This is why I feel it is so important to have a good network of non-physician providers (nutritionists, physical therapists, counselors, etc.) who can help when conventional therapy can’t. We’re all in this together, after all.
Have you been feeling fatigued lately? Do you feel your sex drive isn’t as high as it used to be? Are you having hot flushes, night sweats, or feeling irritable? Maybe your hair is falling out, or is it growing in places you wish it wasn’t? Well friends, a hormonal issue may be at the root of your problem. In this blog series we’ll look at the hormonal causes of symptoms such as those listed above, and what to do about them. So without further do, let’s get started!
In this week’s blog, we’re going to be talking about hormonal causes of weight gain, as well as answering some weight-related questions. Before we get started, however, do you realize how big the weight loss industry is? An article in Business Wire in 2019 stated that the weight loss and diet control market in United States was worth around $72 billion – that’s more than the NBA, NHL and MLB combined! From fad diets and over-the-counter weight loss supplements to prescription weight loss medication and bariatric surgery, there’s no doubt that weight loss is a huge moneymaker in the United States. This may not surprise you, however, as a recent study stated that that roughly 70% of Americans are overweight or obese (defined by a BMI of 25 or greater (BMI is a whole other issue, and honestly we shouldn’t be using it for anything, but that’s another blog, too)), and while we’re doing better as a society in terms of promoting a positive body image, if the above numbers mean anything, many of us still would rather be thin (if you’re interested in the “why” behind this, here are some interesting links).
Regardless, the vast majority of people struggle with weight issues at some point in their lives. In terms of unwanted weight gain, multiple factors contribute to this – a decrease in activity level, dietary choices, lifestyle changes, and so on. But what about those people who gain weight even in the face of dieting and exercise? Or, on the other hand, the people that eat anything they want, sit on a couch all day, and are still the same size they were when they were in high school? There’s more to this whole weight gain thing than simply calories in versus calories out, and that, my friends, is what we’re going to talk about today.
Metabolism and Weight
In order to understand weight gain, or weight loss for that matter, you have to understand metabolism. Put simply, metabolism is the rate in which we make, store, and consume energy. People with a high metabolism tend to burn through energy quicker, and the converse is true for people with a lower metabolism. Many things influence metabolism, such as age, health status, or biologic sex. You can find your basal metabolic rate (BMR), i.e. the number of calories you burn throughout the day at rest, utilizing the following formula :
Women: 655 + (4.35 x weight in pounds) + (4.7 x height in inches) – (4.7 x age in years)
Men: 66 + (6.23 x weight in pounds) + (12.7 x height in inches) – (6.8 x age in years)
You can then take that number and multiply it by various modifiers depending on your overall activity level. Here’s a link to an online calculator, in case you don’t want to do the math on your own.
So using this logic, if we calculate our BMR – let’s say it’s 1600 – and we consume less than 1600 calories in a day, we have a caloric deficit. If we’re able to keep this deficit going, we will lose weight. Sounds pretty straightforward…although this isn’t always the case. I can’t even begin to count the number of times I’ve heard “I’ve tried dieting, counting calories, AND exercising, and the weight just doesn’t come off,” or, the even more frustrating statement, “I’ve tried dieting and exercise, and I GAIN weight.” Obviously this is very annoying, not to mention expensive if you’re using any type of subscription weight-loss service. So what do we do next? Well, let’s look at metabolism (and weight gain) from a hormonal perspective, and see how that plays into things.
Metabolism and Hormones
As previously stated, numerous factors influence our metabolism. Hormonally speaking, however, the number of key players are relatively low. Let’s take a quick look at each of them. As a side note, there are many other hormones that influence weight gain, and we’ll get to them a little later.
Insulin: Probably the most important hormone in terms of carbohydrate metabolism, insulin is produced by the pancreas, and affects blood sugar levels. Without getting into too much biochemistry (if you’re in to that, here’s a link), insulin allows glucose (blood sugar) to pass into cells and either be burned for energy, or stored for further use. This is, in essence, a lock and key mechanism. Insulin “unlocks” cells to allow glucose inside, providing those cells with necessary energy. When the cells won’t open for glucose, the glucose is instead stored as fat. This is the main mechanism behind one of the most insidious aspects of weight gain, insulin resistance. Insulin resistance plays a role in multiple conditions, such as diabetes, PCOS, and Metabolic Syndrome, to name a few.
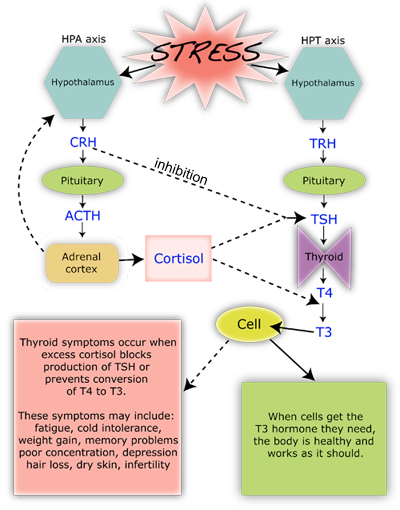
Cortisol: The adrenal glucocorticoid cortisol is the most potent “stress hormone” in our body. It is secreted when our brain perceives we are under stress, be it emotional, physical, or otherwise. Honestly it doesn’t matter if you’re actually under stress or not, if your brain thinks you are, it’s going to tell your adrenal glands to start pumping. From a metabolic standpoint, cortisol activates the sympathetic nervous system (our “fight or flight: response) which causes metabolism to increase, allowing our body to burn through stored energy. In addition, it inhibits the effects of insulin, thereby causing an increase in blood sugar. This is a protective mechanism, as many organs, especially the brain, need glucose to function properly, especially in a high stress situation! Once the stress has resolved, cortisol production decreases, and insulin rises, thereby allowing blood sugar levels to return to normal. In short bursts, this process works wonderfully. With continued, chronic, stress, however (remember, this is perceived stress, too), long-term consequences can arise (see chart below).
Thyroid hormones: The thyroid is in charge of basal metabolic rate. Two main thyroid hormones-thyroxine (T4) and triiodothyronine (T3) are used to increase and decrease metabolic activity as needed throughout the body. T4 is a storage hormone, it is not technically active within cells until an iodine group is removed, and it changes into T3. Let’s look at a diagram…
As you can see above, corticotropin releasing hormone (CRH) blocks TSH production, and excess cortisol effects not only TSH, but the conversion of T4 to T3 as well. In other words, chronic stress affects (via cortisol) thyroid hormone production, and in chronically stressed individuals metabolism is decreased.
So What About Weight Loss?
OK, so we’ve talked a lot about metabolism, and looked at the hormones that affect it. So what about weight? Well, while a higher metabolism can lead to weight loss, just because someone has a higher BMR doesn’t mean that they’ll naturally be thin. Weight loss is a very complicated issue, and as we’ve seen above, metabolism is only a small part of the equation.
I asked my Facebook followers if they had any specific questions about weight loss and hormones, and the response was fantastic. I’d like to answer all of them so for the rest of the blog, so I’m going to do more of a Q&A format. I’ll be including links with these questions, so if you’d like more information on a particular topic, check those sites out!
Q: How do I know my weight issues are hormonal in nature?
A: The short answer is that weight gain/loss is, by nature, a hormonal effect. Aside from the above listed hormones that effect metabolism, there are a multitude of other hormones that influence how our body stores energy. Let’s look at a few:
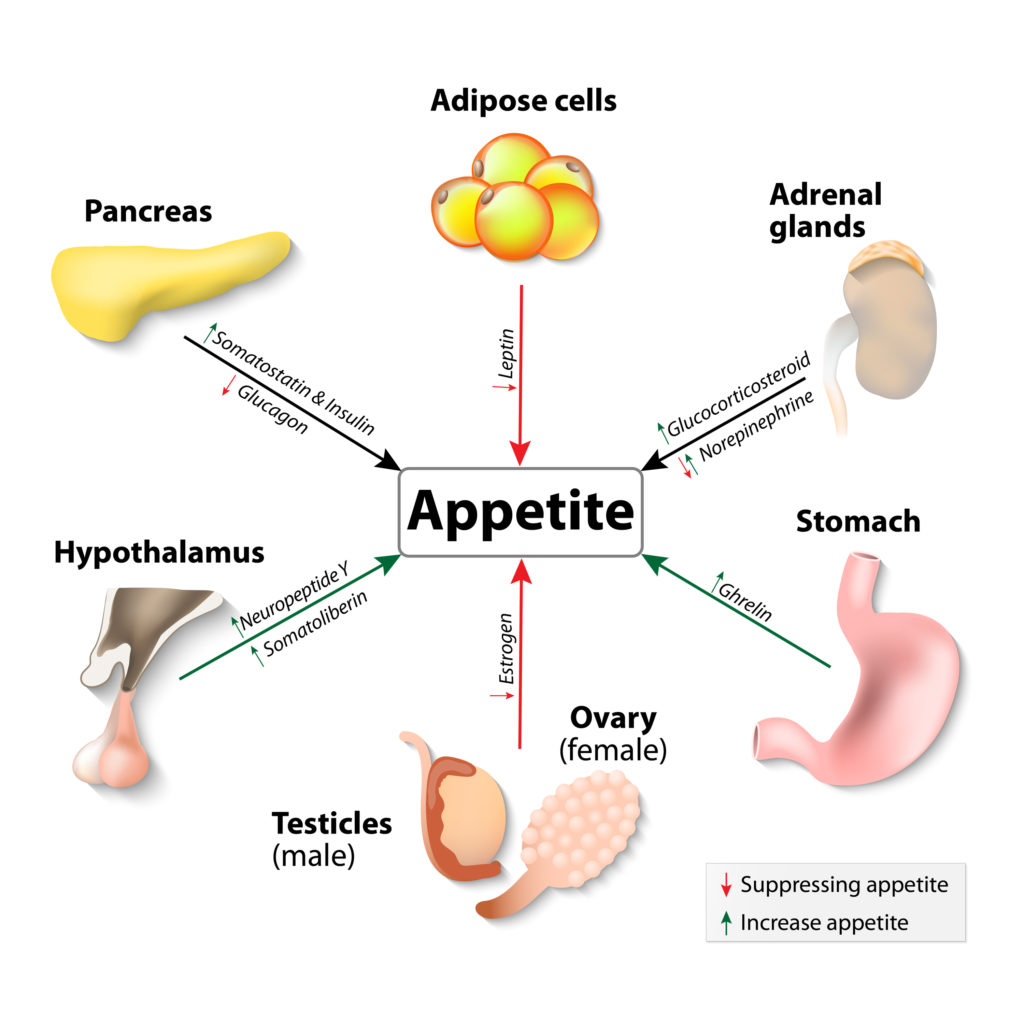
Leptin: Leptin is produced in our fat cells (which means it’s affected by insulin), and is considered a “satiety hormone.” When released, it tells your brain that you have enough fat storage, and therefore helps prevent overeating. Interestingly, obese people tend to have a higher circulating amount of leptin in their blood, which points towards leptin resistance as a possible cause of overeating-related obesity. In addition, leptin is reduced with weight loss, which in essence causes your brain to think you’re starving, which is why it’s so hard to keep the weight off after you lose it!
Ghrelin: In contrast to leptin, ghrelin is a “hunger hormone,” and is produced in the stomach. As you might expect, ghrelin levels are highest right before eating, and drop about an hour after you’ve finished munching. In obese individuals, however, research has demonstrated that ghrelin levels may be abnormally low and that they don’t change as much after eating. This abnormal hormonal behavior is thought to be related to elevated circulating insulin levels, which seem to antagonize ghrelin production.
Estrogens: The estrogen family of hormones plays a role in fat storage and deposition. In times of high estrogen production (puberty, early pregnancy) the body shifts fat cells to subcutaneous areas (namely the hips, breasts, and buttocks) and away from deep, visceral (and abdominal) storage. This relocation of adipose tissue is responsible for the “female form,” and explains why women may lose fullness in those areas after they go through menopause. Increased estrogen intake, be it from birth control pills, hormone therapy, or phytoestrogens (flax, soy) may cause the body to go into a fat-storage mode, contributing to weight gain and obesity.
Peptides: Both Neuropeptide Y (NPY) and Glucagon-Like Peptide-1 (GLP-1) affect our desire to eat. NYP is secreted in times of stress, and stimulates our appetite for carbohydrates (which are rapidly converted into blood sugar). Higher protein intake, as well as prebiotic fiber supplementation may be beneficial in reducing NPY release. GLP-1, on the other hand, is produced in our gut when nutrients enter the intestines, and helps regulate fullness. Chronic inflammation has been shown to reduce GLP-1 production, leading to a decreased since of satiety, which may be a reason so many of us eat when we’re stressed!
Q: Why do some women gain weight after a hysterectomy?
A: This is a very common question. First of all, a hysterectomy is a surgical procedure in which the uterus is removed. A complete hysterectomy involves the removal of the uterus and cervix, and a partial hysterectomy is the removal of the uterus alone-the cervix is left intact. From an anatomic standpoint, the uterus does not produce any substantial level of hormone on its own, but rather has a multitude of hormone receptors. Its removal, therefore, shouldn’t cause any substantial hormonal symptom. So what about post-hysterectomy weight gain? While the reasons for undergoing a hysterectomy are many, most women will have a decrease in activity following surgery. This by itself could lead to some short-term weight gain, but once the “all clear” is given to resume normal activities, that weight should come off. What typically causes hormonal symptoms, however, is when the hysterectomy is accompanied by an oophorectomy, or surgical removal of the ovaries. This puts patients into a iatrogenic, or physician induced, menopause. We’ll discuss menopause in detail in a future blog, but the take-home message is that metabolic activity slows after the menopausal transition and estrogen levels decline, causing a shift in fat distribution as stated above. In addition since endogenous testosterone is also decreased after menopause, muscle mass is lost, and the body’s ability to burn fat and excess calories diminishes.
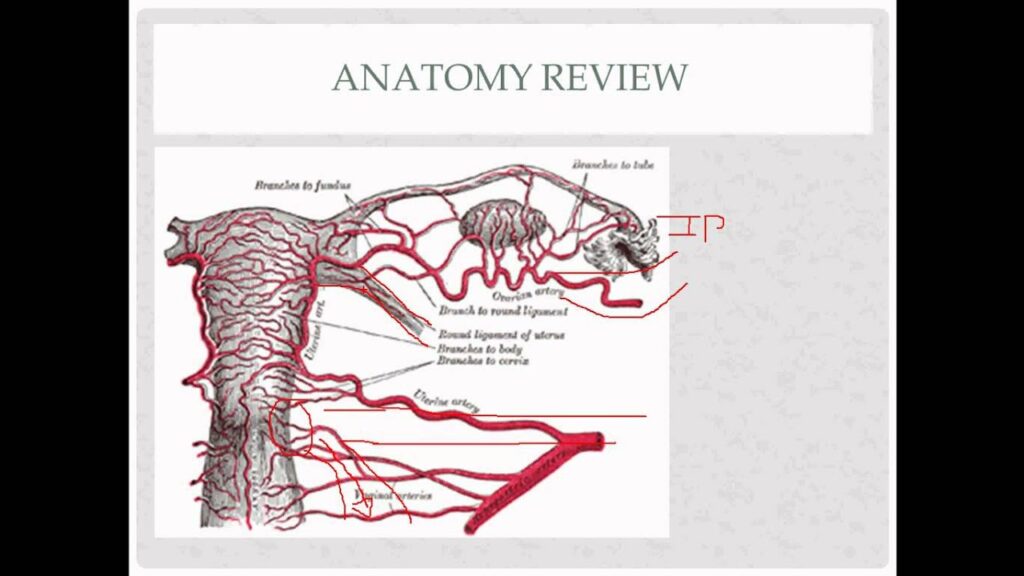
Now I have had patients come in and complain of menopausal symptoms following their hysterectomy, even if the ovaries were left in place. There isn’t really a good medical explanation for this – the research is contradictory. My opinion, however, is when you have multiple patients complaining of the same symptoms following a procedure, there has to be some truth to it. My hypothesis (which is similar to that first study) is as follows: The ovaries received collateral circulation from the vasculature that surrounds the uterus (see picture below). Removal of the uterus can cause a decrease in the blood flow to the ovaries, although not in a substantial enough quantity to cause severe tissue damage. The decrease in blood flow is enough, however, to decrease overall ovarian perfusion, and therefore ovarian function, and decreased ovarian function leads to menopausal symptoms.
Anyone interested in a research study? Let me know!
Q: Can hormones keep me from gaining weight?
A: This is another interesting topic. If you are the type of person that can’t seem to gain weight, no matter what you eat, hormones can definitely play a role. If we rule out obvious hormonal causes such as hyperthyroidism (which boosts metabolic activity), we have to look at those same hunger and fullness hormones listed above. Abnormal levels of Ghrelin and leptin may play a role in people who are chronically thin. Another, albeit not necessarily hormonal cause, would be nutrient malabsorption. Issues with gluten sensitivity, or nutrient and enzymatic deficiency can keep the gut from extracting calories and fats from food, thereby keeping caloric intake low. While this may seem like a “blessing,” nutrient deficiencies and malabsorption actually cause a slew of other symptoms, such as abdominal pain, bloating, as well as diarrhea. If you feel that you are suffering from this condition, I would definitely seek expert care with a gastroenterologist.
Q: Why is a low carb diet good for PCOS?
A: This is an easy one. Many women with polycystic ovarian syndrome also have insulin resistance. In fact, it’s insulin resistance that causes the majority of PCOS symptoms, such as increased facial hair, acne, abnormal bleeding, abdominal weight gain, and oily skin. When insulin levels go up, they suppress Sex Hormone Binding Globulin (SHBG), a regulatory hormone whose sole purpose is to keep free, or unbound, hormones from circulating unchecked. If SHBG is low, then free estradiol and testosterone can run amuck, causing the above stated symptoms. As previously discussed with the insulin paragraph, insulin is responsible for carbohydrate metabolism. Foods that are high in carbohydrates, or more importantly that have a high glycemic index – a measurement of how fast the food is metabolized into glucose – cause a surge in insulin, which over time can lead to insulin resistance. The take-home message for women with PCOS is to try and avoid high glycemic index food. Here’s a list from the American Diabetic Association of foods that have a low glycemic index. We’ll talk more about PCOS in future blogs.
Q: What’s with weight issues and breastfeeding?
A: As to why some women lose weight with breastfeeding, remember that breastfeeding burns an additional 500 or so calories a day. This is because your body is breaking down fat in order to make breastmilk. On the other hand, some women report that they either gain weigh during breastfeeding, or hold onto the weight until they’ve stopped nursing. This is most likely due to either a decrease in activity level, an increase in stress, decrease in sleep, or any combination of the above. In addition, prolactin – the hormone responsible for lactation -causes a down-regulation of estradiol levels. Much like a menopausal woman, a lactating mother will have lower estradiol levels compared to a woman of her same age who is not nursing. This estrogen depletion can cause weight gain as discussed above. I should also state that not eating enough while nursing can lead to weight gain (and a decrease in milk production), as your body goes into “starvation mode,” and holds onto any residual fat stores it has.
Q: Can chronic inflammation lead to weight gain?
A: Of course! Remember cortisol, the body’s most important stress hormone? Well in chronic inflammatory states, our body perceives that inflammation as a stressor, and sends out endogenous corticosteroids to try and reduce it! If you look back up at the graphics, we see that excessive cortisol production not only reduces our ability to utilize insulin effectively, but it also downregulates thyroid function. The end result is more fat deposition, and lowered metabolic activity.
Q: If I’m menopausal (or close to it,) why can’t I lose weight?
A: The menopausal transition brings with it a significant hormonal shift. As a stated above, metabolic activity begins to slow as estrogen and androgen (testosterone) levels naturally decline. A good number of women also report just “feeling worse” during menopause – their sleep quality decreases, they may experience more aches and pains, and they may feel more fatigued, all of which may lower their activity level. This may lead to a multitude of hormonal sequelae, such as:
-Sleep deprivation, which leads to increased stress, which leads to insulin resistance, which leads to weight gain.
-Increased fatigue, which leads to decreased energy, which leads to lowered metabolic activity, which leads to weight gain.
The possibilities go on and on. Keep in mind that as we age our likelihood of developing chronic health conditions rises too, and the diagnosis of something like diabetes mellitus, hypothyroidism, or osteoarthritis can lead to a decrease in activity level as well.
So What Do I Do Now?
Weight loss is a highly controversial, and complex topic, and for me to say something like “let’s just adjust your hormones” downplays how difficult weight loss is. From a medical standpoint, some quicker fixes do exist, such as if someone has insulin resistance, how increasing insulin sensitivity (via diet, medication or supplements) can help shed pounds, or supplementation of thyroid hormone in someone who is hypothyroid. As a general rule though, weight loss is not a simple fix, and in today’s ever increasingly stressful world, it is becoming more difficult to reduce stressors, eat perfectly, and maintain excellent metabolic activity via exercise and supplements.
My advice for those struggling with weight loss is to set realistic goals, and make sure that there isn’t any type of underlying condition hampering your weight loss journey. If you haven’t had a yearly physical, get one – you never know what may turn up. Likewise if there are obvious dietary factors at play (like eating 12 candy bars a day), try and change your diet and see what happens. Additionally, exercise is fantastic, not just for weight loss, but for overall wellbeing and as a stress reliever, and I can’t downplay the importance of a good night sleep, either.
If you’ve done all of those things, and are still struggling with weight loss, you may want to considering seeing a physician who has special training in weight loss therapy. The American Board of Obesity Medicine has a list of physicians who have undergone additional training in the management of weight-related conditions, and is an excellent resource for those patients seeking professional help in their weight-loss journey.
Have you been feeling fatigued lately? Do you feel your sex drive isn’t as high as it used to be? Are you having hot flushes, night sweats, or feeling irritable? Maybe your hair is falling out, or is it growing in places you wish it wasn’t? Well friends, a hormonal issue may be at the root of your problem. In this blog series we’ll look at the hormonal causes of symptoms such as those listed above, and what to do about them. So without further do, let’s get started!
Endocrinology Crash Course
Physiologically speaking, hormones are chemical messengers produced by glands, that fit into specific receptor sites – kind of like a lock and key. When the hormone meets the receptor, a physiologic response takes place. Now keep in mind that these receptors can be all over the body, and that any given hormone can have an effect on multiple types of tissue.
Hormonal symptoms occur when one of the following takes place: the producer gland stops functioning (such as in the case of menopause), there is an excessive amount of hormone produced (what we see in hyperthyroidism), or if the hormone is unable to bind to its receptor (as in the estrogen-blocking effect of Tamoxifen, a medication often used for breast cancer treatment). To complicate things even further, hormone production is regulated by a feedback system – a failsafe, if you will, that attempts to keep too much (or too little) hormone from being produced. If something goes wrong with the feedback system, the downstream effects can be disastrous!
When it comes to treating patients with suspected hormonal disorders, one has to figure out if the issue is with the “producer” or the “target.” Clinical symptoms are often very helpful in determining this differentiation, but as stated above, a singular hormone doesn’t have just one effect. As such, most hormonal evaluations are accompanied by laboratory studies (lots of controversy here). These labs can be performed in a variety different ways, with everything from blood testing, urine testing, or sometimes even salivary or hair follicle testing, to determine the specific value of the hormone at any given time. It is important to note, however, that with a few exceptions these tests provide only a “snapshot in time” of the hormone level in question. As such, a patient may have to undergo multiple laboratory evaluations to get a clear picture of their whole hormonal profile. At this time, serum (blood) testing for sex hormone levels is the recommended method of evaluation and is considered the gold standard by multiple medical specialty societies.
How Hormones are Formed
First things first, that chart above is very intimidating. I remember seeing it for the first time in medical school thinking “holy crap, that’s a bunch of organic chemistry.” I’ve since learned to understand it, but its complexity demonstrates two things:
1: Why endocrinology (hormone disorders) as a specialty exists
2: Why many providers have a difficult time treating hormonal disorders
Now keep in mind that the chart above only shows the sex hormones that are derived from cholesterol. There are literally hundreds of other hormones in the body, but in terms of reproductive functioning, these are the ones that are the most important.
If you look at the color coding on the chart, you will notice some similarities in terms of hormone “families.” Progestogens in yellow, androgens in blue, estrogens in pink, and corticoids in…a color mishmash. The families are based on the number of carbon atoms in the hormone itself, as well as the placement of specific “functional groups,” collections of chemicals that further define the base compound. For example, estrone and estradiol are both made of up 18 carbon atoms (as are all estroGENS), but whereas estraDIOL has two hydroxy groups, estrONE has a ketone group.
I understand this blog is not about organic chemistry, nor would I ever want it to be, so that is about all I am going to say about that.
Hormone Symptom Breakdown
Now that we’ve covered what hormones are, and how they work, let’s look at some hormonal symptoms and potential causes. I’m going to be addressing a good number of these in detail in the upcoming weeks, but for today I thought I would do an overview of many of the hormonal symptoms that I see on a regular basis. As a caveat, the hormones listed below are not the only causes for these symptoms, and as always, this information does not take the place of an actual visit with a licensed provider.
Thoughts: When it comes to weight, you have to look at 2 different things.
1: Metabolism
2: Stress response.
Our metabolism slowly begins to decline once we have 30, due to a very complex assortment of causes, and changes in lifestyle, childbirth, and decreased sleep all can play a role in weight gain. As your thyroid also helps regulate metabolism, a low functioning thyroid can contribute to weight gain, as well. Lastly, stress hormones such as cortisol and insulin, when elevated, decrease your body’s ability to “let go” of fat.
Thoughts: In terms of sexual functioning, testosterone is often the hormone that most people think of. While it is true that low testosterone can cause low sex drive, sexual desire is a very complex subject that is not based on hormonal functioning alone. Sexual pain disorders, especially pain with penetration, can sometimes have a hormonal component. Lastly certain drugs that affect our mood, such as selective serotonin reuptake inhibitors (SSRI’s), can cause a shift in the serotonin/dopamine balance-the neurotransmitters responsible for sexual functioning.
Symptom: Menstrual Mood Disorders
Potential hormonal cause: Changes in estradiol and testosterone
Thoughts: Menstrual-related mood disorders are hormonally due to either a drop in estradiol, or an elevation in testosterone. In the elevated testosterone population, patients often complain of violent, angry outbursts, and in extreme cases, may have had multiple disciplinary actions taken against them at work or school. Conversely, in those with the low estrogen subtype, anxiety, fear, or other avoidance type of activities may predominate.
Thoughts: Elevated androgens – testosterone, dihydrotestosterone, and their precursors (see chart above), are often to blame for unwanted facial and body hair growth, and can cause of a type of hair loss called androgenic alopecia. These symptoms are often found in conditions such as polycystic ovarian syndrome, insulin resistance, and late onset congenital adrenal hyperplasia. Given that the thyroid controls metabolic activity, low thyroid functioning can also result in hair loss.
Well friends, that’s it for the first blog in this series. I hope you enjoyed reading it as much as I enjoyed writing it, and I look forward to delving deeper into different hormonal conditions in the upcoming weeks! As always, if there’s a topic you find interesting, or would like to know more about, let me know!
How much do you know about your anatomy? What is really considered normal? Should we even say that something is “normal?” Well with this series of blog posts, I hope to dispel some of the myths about female anatomy, as well as discuss certain changes in pelvic anatomy that would warrant a visit to your gynecologist.
As always, this post does not take the place for actual medical advice. If you have concerns or questions, please reach out to your provider. That said, to the Pelvis!
For the final blog in our anatomy series, I thought I would focus on a pelvic structure that is so very important to sexual health, but also affects urination, defecation, and overall core and low back support. It is with great joy that I present to you…
The Pelvic Floor
The Pelvic floor is a fascinating group of muscles that form a hammock for your pelvic organs, keeping them in correct anatomic position. Found in both men and women, the pelvic floor is important in sexual function, defecation, movement (through its attachments to the hips and legs), and controlling urination. In women, the pelvic floor allows for the pelvic bones to move during childbirth, and is one of the reasons women are able to deliver vaginally. I should note that most practitioners use the terms pelvic floor and pelvic diaphragm interchangeably, although there is an anatomic difference between the two.
Musculature
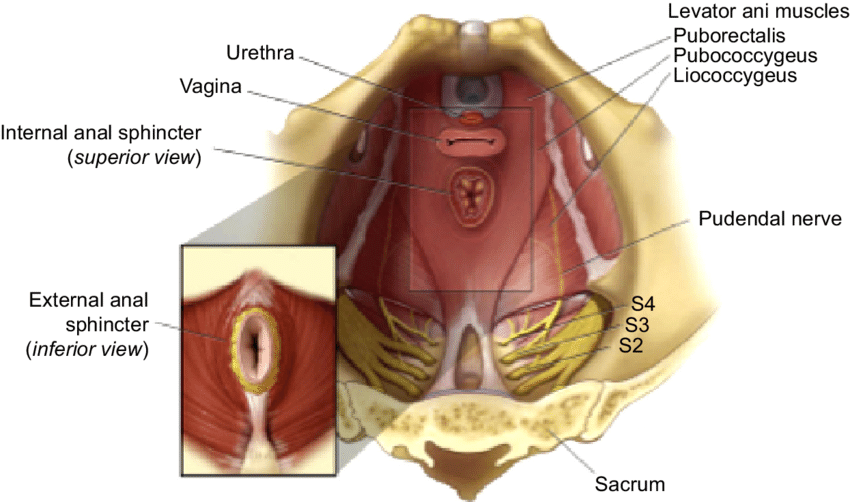
The Pelvic floor is anatomically comprised of two distinct muscle sets, the Levator Ani group (pubococcygeus, iliococcygeus, and puborectalis), and the Coccygeus. In addition, the Obturator internus (which on that diagram above is the white, filmy muscles adjacent to the iliococcygeus), plays a substantial part in pelvic function, too. These muscles work in tandem to aid in all sorts of ambulation and bodily functions, relaxing and contracting as needed depending on the desired action. Like all muscles, they can be damaged, usually during events that cause substantial stretch trauma (such as childbirth), although repetitive stress to the muscles (such as with chronic cough) can cause injury over time, too. In addition, atrophy to the musculature can occur in patients with neurologic conditions, or in very sedentary individuals.
Innervation The innervation (nerve supply) to the pelvic floor originates mainly from the sacrum. Sacral nerves 2,3, and 4 form the pudendal nerve, which in turn descends through the pelvic floor, exiting through Alcock’s canal in the groin. It then branches into a clitoral branch, a perineal branch, and an anal branch, innervating those respective structures. Damage to the pudendal nerve typically occurs at the nerve root (in the sacrum), or where it traverses the pelvic floor. In both cases, trauma is often the cause of the nerve damage, be it from something like a fall, car wreck, or vaginal delivery. In addition, muscles spasms along the pelvic floor can entrap the pudendal nerve, which causes sharp, stinging pain in structures downstream from the entrapment.
Treatment for pudendal nerve issues is tricky, and often involves multiple therapeutic modalities. Medication, nerve blocks, physical therapy, and behavioral therapy often work hand-in-hand, and with good care, significant improvement or resolution of symptoms can be achieved. Rarely is surgery indicated for pudendal nerve dysfunction.
Vasculature The anterior division of the internal iliac artery provides the majority of the blood supply to the pelvic floor. That vessel has three “terminal” branches, the pudendal artery, the inferior gluteal artery, and the inferior vesicle artery, all of which distribute blood to various structures in the pelvis. As with nerves, damage to, or entrapment of, blood vessels cause downstream effects. If a vessels is mildly compromised, the muscles that it supplies will experience “ischemia,” or a decrease in oxygenate blood. This manifests as pain – often dull, or achy in quality. Peripheral blood vessels often try and compensate for this decreased blood flow by bringing more blood to the area, thus creating a reddened or “hyperemic” appearance. This explains why patients with vestibular pain secondary to pelvic floor spasms often have a very red, irritated looking vestibule.
Treatment for vascular-relate pelvic floor disorders is based around restore normal blood flow. This can be accomplished by medications (blood thinners, antihypertensives, etc), physical therapy, or even surgery, especially if congenital malformations that affect the shape and flow of the pelvic vessels are present.
Prolapse I would be completely remiss if I did not talk about pelvic organ prolapse in a blog concerning the pelvic floor. Pelvic organ prolapse is a condition in which the pelvic organs lay in an altered anatomic position secondary to deficiencies in support. There are four main types of pelvic organ prolapse: cystocele, rectocele, uterine prolapse, and vaginal vault prolapse. As each of these conditions warrants a blog itself, I’ll just go over the basics of each type.
A bladder prolapse, or “cystocele,” is a condition in which the bladder falls into the anterior, or top, portion of the vagina and can protrude out of the vagina with increased intra-abdominal pressure (such as coughing or laughing). Symptoms of bladder prolapse include urinary incontinence, urinary hesitancy, or sensation of fullness in the pelvis.
A “rectocele”, or posterior vaginal wall prolapse, is a condition in which the support structures on the posterior aspect of the vagina are weakened, and the rectum is allowed to protrude into the vaginal canal. This can cause a sensation of pelvic fullness, and may lead to constipation. Some women may have to place a finger inside the vagina and help push stool, in a maneuver known as “splinting.”
A uterine prolapse is a condition in which the support structures of the uterus have weakened, causing the uterus to “fall” into the vagina. This typically manifests as low back pain and pelvic pressure, and in some women can cause pain with intercourse or even bowel or bladder problems.
Finally, a vaginal vault prolapse is a condition that occurs after a hysterectomy, in which the apex of the vagina falls from its original position due to a loss of suspensory structures. Typical symptoms of a vaginal vault prolapse are the sensation of heaviness or fullness in the pelvis, as well as a visible bulge at the opening of the vagina.
The Take-Home
Pelvic floor health is so incredibly important. In fact, you could say that pelvic floor health = gynecologic health, at least in terms of pelvic pain, continence, and sexual functioning. If the pelvic floor is not functioning properly, a thorough pelvic floor evaluation needs to be performed. At Haven Center, we do a pelvic floor exam utilizing a bimanual vaginal technique in which we palpate the individual muscle groups, as well as perform a visual inspection to check for prolapse. Should we find an area of concern, the next step in the treatment for these conditions is a referral to a certified pelvic floor physical therapist.
Well friends, this is the end of this blog series. I hope you’ve found it informative, and have a better appreciation for gynecologic anatomy! If you have any questions, don’t hesitate to ask, otherwise I’ll see you with the next blog! Remember – there is hope, there is help, there is Haven Center!
How much do you know about your anatomy? What is really considered normal? Should we even say that something is “normal?” Well with this series of blog posts, I hope to dispel some of the myths about female anatomy, as well as discuss certain changes in pelvic anatomy that would warrant a visit to your gynecologist.
As always, this post does not take the place for actual medical advice. If you have concerns or questions, please reach out to your provider. That said, to the vagina!
Continuing our delve into anatomy, this blog will discuss the vagina. From the Latin word meaning “sheath,” the vagina is a tubular structure, extending from the uterine cervix to the vestibule. It averages approximately 6.2 cm in length, with a width that can vary greatly (as seen in childbirth). Much like the vestibule, its embryologic homologue is the prostatic utricle, and on a cellular level, it is composed of both rigid “parabasal” cells that give it shape and form, as well as flexible, glycogen-containing “superficial” cells that allow it to stretch and withstand trauma.
The vagina has some interesting characteristics. Hormonally speaking, it is rich in estrogen receptors of all types. Estradiol, the most potent form of estrogen, composes the majority of its receptor affinity. A decrease in this hormone, as is seen with menopause, is one of the reasons that many women experience vaginal dryness or pain with intercourse following that transition. Another interesting thing about the vagina is that many medications have a vaginal route of administration. This is because the mucosal lining of the vagina is porous, and allows for dissemination of medication through the walls, and into the bloodstream. Hormonal medications utilize this route of administration quite frequently, but antibiotics, antifungals and even anti-nausea medications will sometimes be given vaginally, as well.
As a whole, disorders that originate from the vagina itself are rare. That said, many gynecologic conditions have symptoms that manifest vaginally, such as the increased vaginal discharge that is seen with cervicitis, or the vaginal pain that often accompanies pudendal neuropathy. A thorough history and physical is often needed to determine whether the cause of the patient’s complaints is due to a problem with the vagina itself, or if the vaginal symptom is just a manifestation of extravaginal disease. What are some of those vaginal disorders? Well let’s take a look!
Some Vaginal Conditions (that actually come from the vagina)
Infectious Vaginitis
By far the most common vaginal condition (that actually comes from the vagina) is vaginitis. Vaginitis is an overarching term, simply meaning inflammation of the vagina, and while there are many different causes of vaginitis, I would like to focus on one of the most common types, bacterial vaginosis (BV). Simply speaking, BV is an overgrowth of normal bacteria within the vaginal mucosa. The most common bacteria involved are forms of Lactobacillus, but other species of bacteria, including Gardnerella, Prevotella, Fusobacterium and Bacteroides are often implicated in this condition as well.
Bacterial vaginosis is not a sexually transmitted infection, although it is often precipitated by sexual contact, and may increase the risk of developing a STI. Other factors such as changes in diet, medications, or alterations in the vaginal pH (such as with douching) can cause the development of BV as well. The hallmark symptom of BV is vaginal discharge. This discharge is often irritating to the vaginal mucosa, and can cause itching or discomfort, and may produce an amine, or “fishy,” odor.
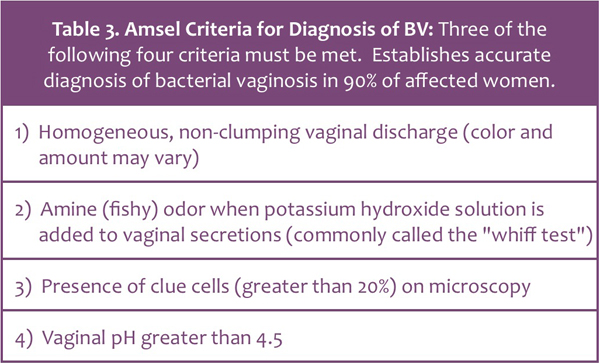
The diagnosis of bacterial vaginosis is rather straightforward, and is based off of Amsel’s criteria (listed below).
Treatment for uncomplicated BV is equally simple, and involves either medication to eradicate the bacterial overgrowth, or dietary/lifestyle changes to improve the vaginal pH/flora. Should these treatments fail to fully resolve symptoms, further investigation is warranted.
Desquamative Inflammatory Vaginitis (DIV) On the other end of the vaginitis spectrum is an noninfectious, inflammatory disorder of the vaginal epithelium, known as desquamative inflammatory vaginitis, or DIV. DIV typically occurs in postmenopausal women, although in my personal practice, I have seen it in quite a few premenopausal patients. The hallmark symptom of DIV is a copious vaginal discharge that is very thick – almost glue-like – in its consistency. A vaginoscopic exam will reveal multiple areas of diffuse redness with yellow-tinged vaginal secretions. At times, small red macules -flat areas of irregular shape – will also be present on the vaginal wall.
Diagnosis of DIV is based off of history, symptoms, and bacterial cultures. A wet-mount preparation will reveal decreased acidity, multiple white blood cells, and none of the normal “good” bacteria. If a bacterial culture is taken, Group B Strep (which is normally not pathogenic) is often found. Treatment for DIV is focused on reducing the inflammatory aspect of the condition, changing the pH, and suppressing any bacterial activity. I typically use a compounded estradiol, clindamycin and hydrocortisone cream for this purpose, although other treatment protocols do exist.
The Take-Home
Honestly, the most important factor when it comes to treating vaginitis is correct identification. BV does not equal DIV, vaginal Crohn’s, or a Chlamydia infection, all which have vaginal discharge as a common symptom. Some practitioners may knee-jerk send in a prescription for an antibiotic when told by their staff that a concerned patient called complaining of vaginal discharge; obviously this is not best practice, and in some cases, may make the symptoms worse. It is my opinion that women with vaginal discharge – especially if it causes pain, itching or other bothersome symptoms – should be evaluated, and the discharge cultured and examined microscopically.
Well friends, that wraps it up for this blog. Next time we’ll examine the pelvic floor in the final installment of It’s All About Anatomy. Until then, have a great week, and don’t forget – there is hope, there is help, there is Haven Center!
How much do you know about your anatomy? What is really considered normal? Should we even say that something is “normal?” Well with this series of blog posts, I hope to dispel some of the myths about female anatomy, as well as discuss certain changes in pelvic anatomy that would warrant a visit to your gynecologist.
As always, this post does not take the place for actual medical advice. If you have concerns or questions, please reach out to your provider. That said, to the vulva!
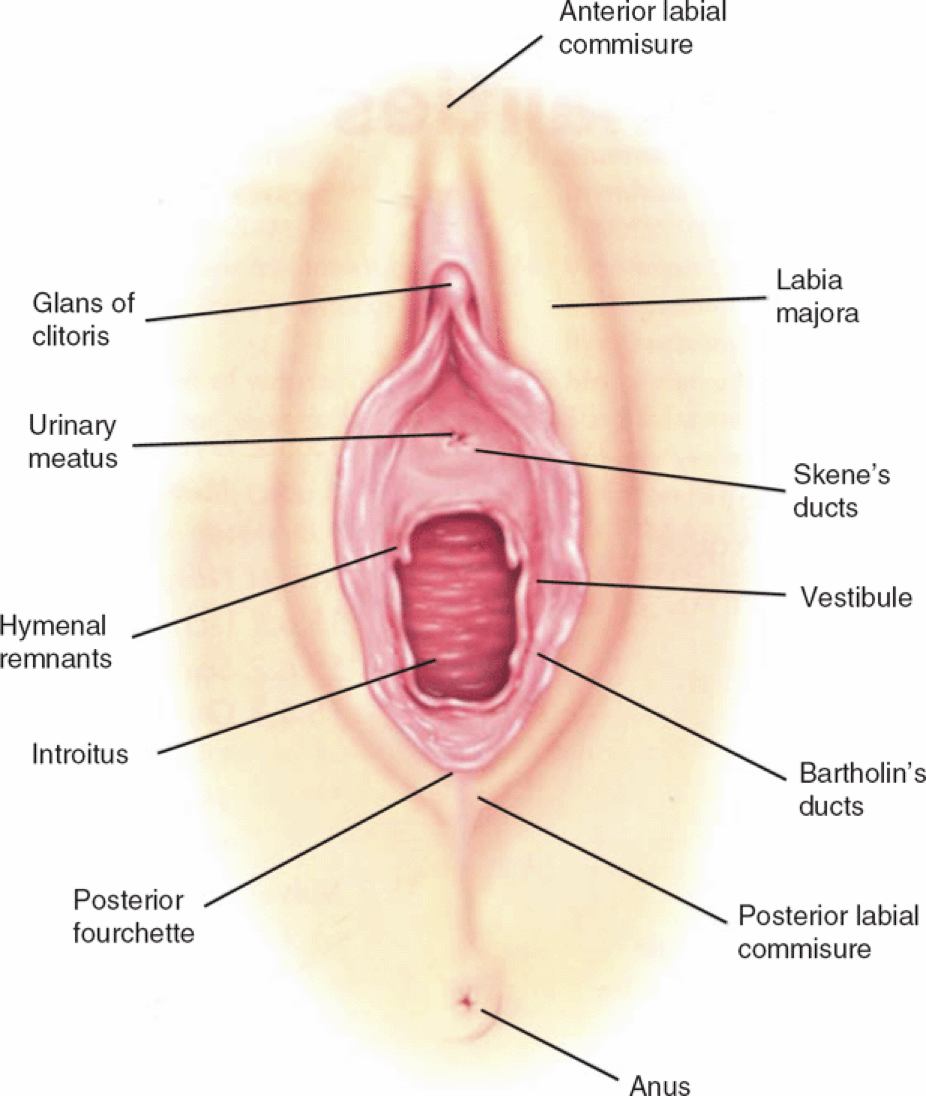
In this week’s blog, I’m going to talk about an oft’ forgotten portion of the vulva, the vestibule, also known as the Vulval Vestibule (archaic term), the Vulvar Vestibule, or the Vestibule of the Vagina. As you can see in the image above, it hasn’t even been marked – which is a travesty, given how important the vestibule is in terms of sexual health. Let’s try again…
There we go. Much better.
Anatomy
The vestibule is anatomically delineated from Hart’s Line on the labia minora to the Hymenal opening/remnant. It forms from the most distal portion of the urogenital sinus, and as expected, has a male homologue – the prostatic utricle. In addition, the vestibule is the home of the urethra, the paraurethral glands (Skene’s glands), and the Bartholin Glands. It also contains the hymen, the thin membrane that partially covers the opening of the vagina itself.
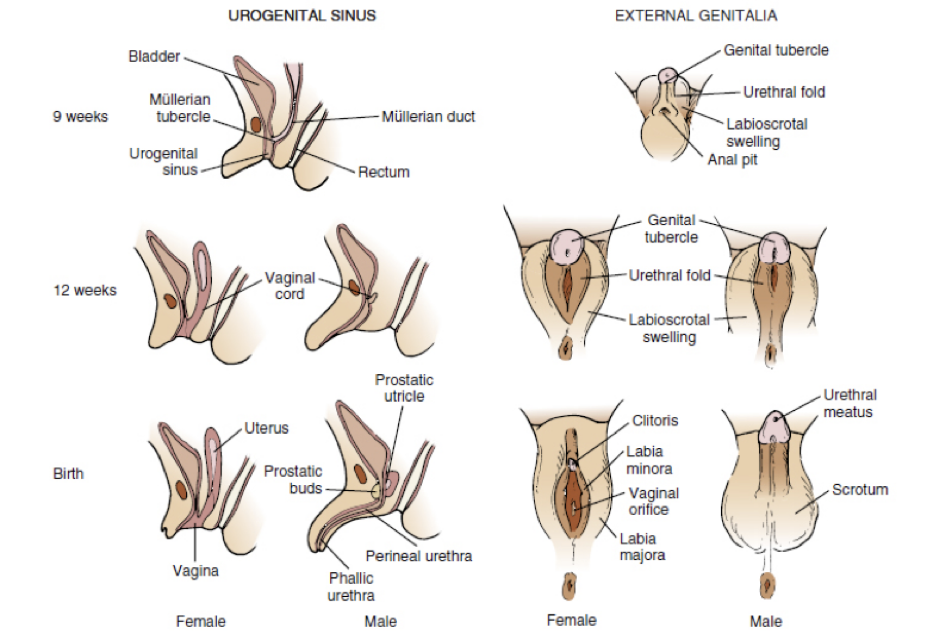
One of the most interesting things about the vestibule is that it is very dense with androgen (testosterone) receptors. This is because both the vestibule, and the prostatic utricle, originate from the same urogenital sinus, an area rich in both androgen and estrogen receptors. As the fetus continues to develop, the vestibule becomes a separate anatomic structure, but due to its origin, it retains its sensitivity to those hormones. Phew! If you’re more of a visual learner, here’s a picture that basically shows that embryologic differentiation.
Regardless of what type of learner you are, the take home message is this: both estrogens AND androgens are necessary for vestibular health. This is incredibly important when it comes to addressing vestibular complaints. What are some of those complaints, you ask? Well let’s take a look!
Common Vestibular Complaints
Pain: By far, the most common vestibular complaint is pain. The vestibule is rich with nerve endings, and is very sensitive to both pain and pressure. Vestibulodynia, a word that literally translates to “pain in the vestibule,” is the medical terms for…well…pain in the vestibule, and has many potential etiologies, such as bacterial/fungal infection, nerve hyperstimulation, and hormonal deficiency.
Itching: Vestibular itching is often due to an infectious process. Yeast infections, commonly caused by the fungus Candida albicans, are a very common cause of itching, and often respond quite well to antifungal therapy. That said, while over-the-counter therapy may be a quick and easy way to treat most yeast infections, it doesn’t always work. In my opinion, women with recurrent yeast infections should have a culture taken to determine the exact strand of yeast that is causing the problem, so that the correct antifungal medication can be prescribed. In addition, some women colonize yeast in their rectum, and will have recurrent fungal infections despite vaginal anti-fungal therapy. In this case, a different antifungal – one that is active in the intestine/colon – is needed to help eliminate the problem.
Painful intercourse: Vestibulodynia is often a cause of dyspareunia, or painful intercourse. In my reproductive-age patients, a hormonal vestibulitis – caused by long-term oral contraceptive (OCP) use – is one of the most common causes of painful intercourse I see. A large number of OCPs cause Sex Hormone Binding Globulin (SHBG), a hormone that binds free sex hormones (thyroid hormones, too) to be excreted in high amounts, thereby lowering the amount of available estradiol and testosterone. As stated above, the vestibule requires estradiol and testosterone, and without those sex hormones, it becomes irritated and inflamed, and thus, painful if stimulated. Treatment is based around stopping the oral contraceptive use, as well as correcting those estradiol and testosterone deficiencies.
This is by no means an exhaustive list of vestibular complaints. So if you or someone you know has one (or all) of the above symptoms, please reach out! There is soooo much that can be done to improve these conditions. It’s an unfortunate truth that many healthcare providers don’t understand vestibular disease, so expert consultation is important!
Have a wonderful week, and don’t forget – there is hope, there is help, there is Haven Center!
How much do you know about your anatomy? What is really considered normal? Should we even say that something is “normal?” Well with this series of blog posts, I hope to dispel some of the myths about female anatomy, as well as discuss certain changes in pelvic anatomy that would warrant a visit to your gynecologist.
As always, this post does not take the place for actual medical advice. If you have concerns or questions, please reach out to your provider. That said, to the vulva!
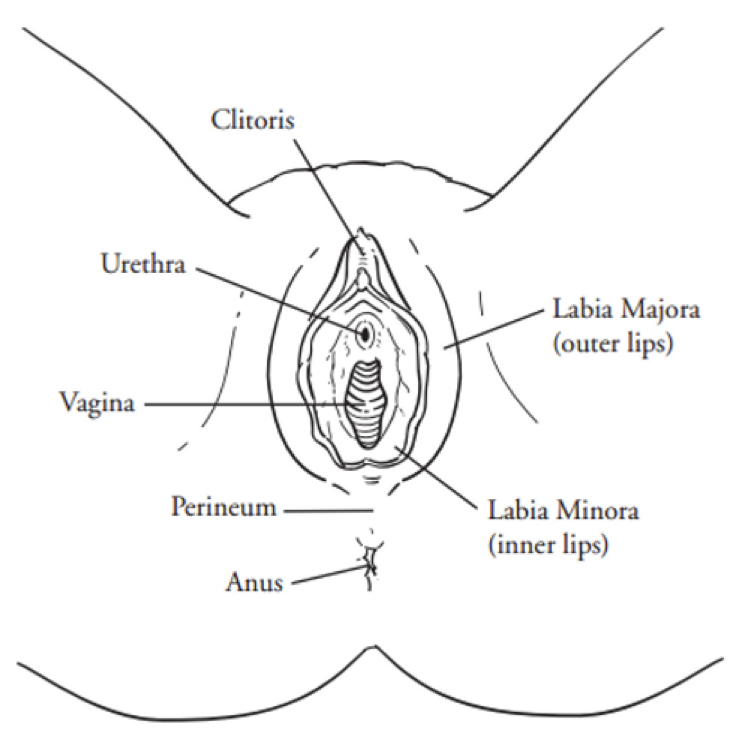
In this week’s blog, I am going to discuss the labia. As you see in the picture above, there are two distinct sets of labia, the labia majora and the labia minora. The word labia comes from the Latin word for “lip,” with majora meaning “the larger,” and minora, meaning “the smaller.” I should also point out that labia, majora, and minora are plural nouns. The singular form for those structures are labium, magus, and minus, respectively.
The Anatomy of the Labia
From an anatomical standpoint, the labia majora are cutaneous folds that extend from the mons pubis (a fat pad that sits atop the pubic bone) to the perineum (the area between the vulva and rectum). They contain a number of sebaceous (sweat) glands, as well as other structures, such as hair follicles. As hormonally-sensitive structures, they are rich in estrogen receptors, and consequently, will change size and shape with puberty and menopause. Embryologically, they are an anatomic homologue (remember that term from the clitoris blog post?) to the scrotum, and are derived from the labioscrotal folds which, as a female embryo develops, split down the middle, forming the pudendal cleft. Pretty straightforward, right? Now here’s an interesting tidbit (that unfortunately leads into the next section), the word pudendum comes from the Latin word for “Shame.” There’s no doubt that the original anatomists who created the terms for our body had issues with female anatomy, but it seems…shameful…that they would name it so. Maybe this is why prior to the 20th century, virtually no art depicted female genitalia.
I guess you could say that historically, human beings have an issue with labia.
The Controversy
Skip to the 21st century. From vilification (female genital mutilation) to exaltation (the pornography industry), we can’t seem to leave labia alone, and whereas people of the past may have only seen a few sets of labia during their lifetime, it’s become easier than ever (thanks to the internet) to have a plethora of pudenda to compare oneself to. As you may imagine, this constant comparison can lead to feelings of inadequacy, frustration, or that one’s own anatomy is not “good enough.” And how do we fix this?
Enter the labiaplasty.
Technically speaking, a labiaplasty is a surgical procedure that changes the shape, form, or size of the labia. It is currently considered (for most women) a cosmetic procedure, and therefore is often not covered by commercial health insurance. Nevertheless, more and more women are seeking surgery. According to the American Society of Plastic Surgeons, the number of labiaplasties have skyrocketed since the Society began collecting that information in 2015, and a quick google search for “Labia surgery” will direct you towards a multitude of plastic, cosmetic, gynecologic, and cosmetogynecologic surgeons willing to perform the procedure (some with better qualifications than others). As to why some women desire labiaplasties, issues with personal hygiene, symmetry, cosmetic appearance, or even wearing “cuter clothes” make the top of the list, although a few sites I searched listed some variation of “getting back to being normal” as a potential reason for undergoing surgery.
I had to reread that a few times. “Getting back to normal,” eh? Who gets to decide that?
Over the last few years there has been an outpouring of voices discussing “normality” of the labia in terms of size and shape. Various online publications, both health-related (Healthline.com, Medical News) and otherwise (Cosmopolitan Magazine, Women’s Health magazine) have chimed in on this debate, and even the American College of Obstetricians and Gynecologists (ACOG) has made a stance on “normal size.” All in all, the take home message is the same: there is no “normal” in terms of labial size. Each set of labia, much like each woman, is unique. Furthermore, the labia don’t have to be symmetrical – one can be larger than the other, and still be completely anatomically “normal.” To further this point, Laura Dodsworth, a British photographer and author of Womanhood: The Bare Reality, photographed over 100 different vulvas in an effort to display the complete variety of anatomy that exists. Her message: there is no normal. Your anatomy, in whatever shape and size, is perfect.
There is, of course, a rebuttal to this argument: just because there isn’t a “normal,” doesn’t mean labia can’t be bothersome. I’ve personally had patients who feel embarrassed by their labia, or who complain they get caught in clothes, or are injured during intercourse. For these patients, surgery can be a lifechanging (in a good way) thing. Obviously surgery is not without risks, and careful attention to detail, as well as appropriate postoperative expectations is important.
But this begs another question – why are we even having this conversation about cosmetic labial surgery? If I didn’t like my nose, would anyone fault me for having a nose job? Sure, maybe it would help me breathe better, but really, maybe I just don’t like my nose. What about breast augmentation? If a woman has symmetrical, yet small breasts, is her desire to increase her cup size any less important/valid than the same desire in a woman with one C cup, and one AA cup?
The Take-Home
Our self image IS important, and no man, woman, or otherwise should have their desire to “look their best” invalidated. And yet, in terms of labia, if you look at the statistics, the vast majority of woman have labial shapes and sizes that are numerically within the” normal” range. In my opinion, if a woman desires a labiaplasty, whatever the reason, I think she should be able to have one, as long as it is performed in a safe and professional manner. I do take issue, however, with surgeons who prey upon genital insecurities, or who claim that the surgery is without any potential for complication or long-term issue. My take home message – if you’re going to have surgery, do your homework. Honestly, if you’re going to see any medical provider, do your homework.
I guess you could say, take charge of your own health! And remember – there is hope, there is help, there is Haven Center!
How much do you know about your anatomy? What is really considered normal? Should we even say that something is “normal?” Well with this series of blog posts, I hope to dispel some of the myths about female anatomy, as well as discuss certain changes in pelvic anatomy that would warrant a visit to your gynecologist.
As always, this post does not take the place for actual medical advice. If you have concerns or questions, please reach out to your provider. That said, to the vulva!
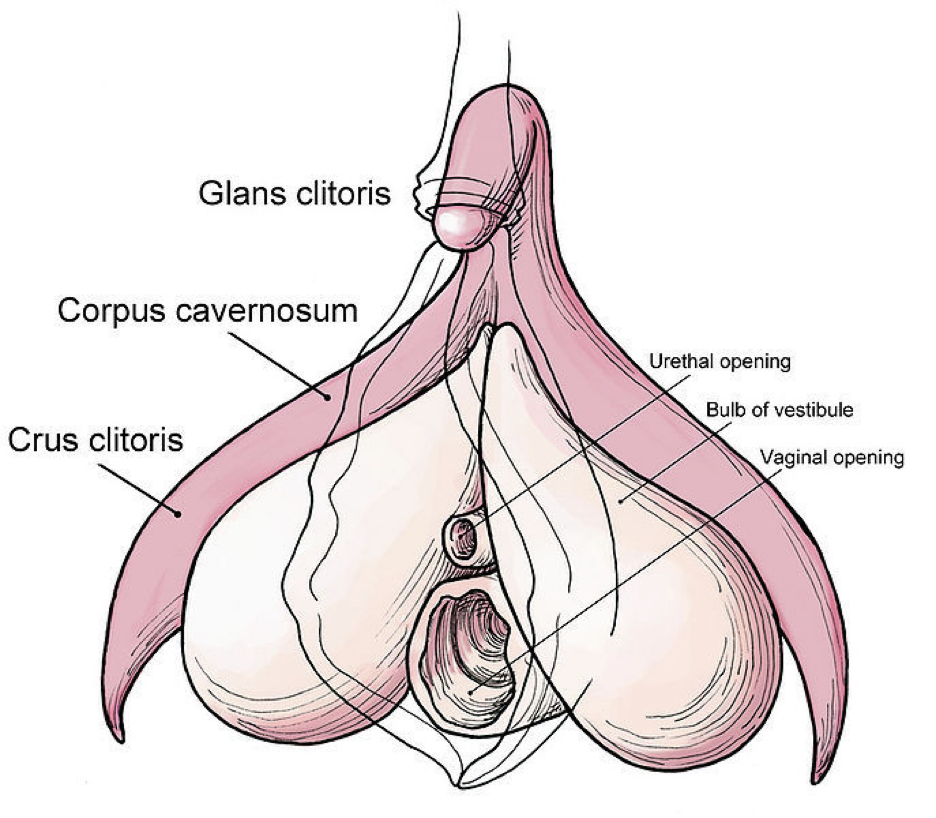
This is a very black and white, textbook illustration of the external female genital tract. I would be remiss if I didn’t point out that the vagina is only a small part of this entire structure. As a society, we colloquially refer to the female genitalia as the “vagina” for some reason, but in reality it is a very specific section. More on that later..
This week, we’ll be starting from the top. I present to you…
THE CLITORIS
This is an impressive structure. If you know anything about male anatomy, you will see some correlations in the names of certain structures, namely the corpus cavernosum, as well as the glans. This is because the clitoris is what is considered an anatomic homologue, a structure that has a equivalent in the opposite biologic sex. The crazy thing about the clitoris is that it has only recently been fully examined in terms of innervation, vascularity, and structure, and by recently I mean since the 90’s (with most articles published after 2000). This journal article, which was published in 2005, is one of the first to fully “…present a comprehensive account of clitoral anatomy, including its component structures, neurovascular supply, relationship to adjacent structures (the urethra, vagina and vestibular glands, and connective tissue supports), histology and immunohistochemistry.”
Just for reference, I was in medical school in 2005 and “Holla Back Girl,” was resting at #2 on the Billboard Hot 100 list.
I would also point out that the article discussed above was published in a Urology journal, not Gynecology. This is a huge issue, because as gynecologists, we are supposed to be THE expert in female anatomy. To compound things even further, until very recently, no gynecologic textbooks mentioned specifics about clitoral anatomy (length of nerves, vascular compliance, etc.). As to why this is…well, that’s a great question. Maybe it’s due to what Jessica Pin, (one of the lead authors of the study that pushed detailed clitoral anatomy into certain GYN textbooks) reported as “…sociocultural discomfort with the clitoris and a pervasive lack of regard for female sexual response (seen as a bonus rather than necessity), as it is not legitimized by direct reproductive function.” Maybe it’s a decision of whom Dr. Jen Gunther calls the “Patriarchy,” the oppressive consortium of medical policy makers that define what is, and what is not, important in women’s health. Or maybe it’s simply an oversight on the part of medical textbooks editors and physician educators for the last, oh, 1000 years?
Regardless, the clitoris has an important role in women’s sexual health, and overall sense of wellbeing. It is, therefore, incredibly important for women’s health providers to understand the anatomy, as well as function of the clitoris, especially in patients that present with complaints regarding that organ.
What are some of those complaints, you ask? Well, here is small collection of common clitoral concerns!
Clitorodynia: An overarching term that basically means pain in the clitoris. Clitorodynia may be due to clitoral adhesions, vascular insufficiency, keratin pearls, neuropathies, or a multitude of other conditions.
Clitoral Adhesions: Clitoral adhesions are scar-like tissue formations that form between the glans of the clitoris and the clitoral hood. This may lead to tenderness or itching in the clitoral area, and can be a cause of painful intercourse, pelvic pain, or even Persistent Genital Arousal Disorder (PGAD). In certain cases, these adhesions can lead to the formation of small keratin collections called keratin pearls.
Clitoral Retraction: Clitoral retractions may occur with conditions that cause sex hormone level to be low, such as menopause or long-term oral contraceptive use, or in vulvar skin conditions such as lichen sclerosus. A retracted clitoris can be tender, and may lead to significant discomfort with sexual activity.
Clitoral Itching: Often associated with vulvar dermatoses, clitoral itching can be a symptom of multiple conditions, including cancer of the clitoris itself. Persistent clitoral itching, as with any type of persistent genital itching, should be investigated.
Well friends, that’s all I have for you today. I hope you enjoyed the first of this blog series. As always if you have any questions or concerns, please let me know.
Have a wonderful rest of your day, and remember – there is hope, there is help, there is Haven Center!
We have been discussing neurodivergence and Gynecology- specifically looking at ADHD as well as the autism spectrum disorders in terms of hormonal functioning sexual functioning basic Gynecology things kind of everything that’s in there now obviously the preamble to this video is that there is not a lot of data out there about these conditions and the specific topic you know in terms of sexual medicine for example I mean the you know the whole specialty is honestly kind of new-ish and you know these things represent the the there be dragons kind of you know aspect of the map of what’s going on with with sexual medicine so there’s lots of stuff coming down the pike there’s but there’s not a lot of of information to to pull data statistics from.
The idea of neurodivergency or neurodifferential processes comes from the thought that patients who have these types of conditions are interpreting data in a different way than the averagel person and whether that means that the neurons in the brain are firing differently whether it means that they are kind of interpreting you know the input of of stimulation differently whatever it may be it’s considered kind of a Divergent way of of dealing with this input of data and so when you look at that there is a huge spectrum of this and and obviously you know we’re just talking about two different things today, but even within those two different areas there’s lots of degrees there too
There’s so muchdata to be found kind of in this this sub-area of of mental health and medical health that is really unique and interesting.
ADHD or attention deficit hyperactivity disorder has gone through a lot of different names for the condition. For a long time this was just thought to be people that couldn’t sit still – maybe they had a hard time concentrating, maybe they were fidgeters… typically the kids that are ‘bouncing Off the Wall’, and there wasn’t a lot of thought put into it.
Times have changed- we have learned a lot more about the diagnosis… we’ve learned that you know there’s a broad variety of different treatments for patients with these conditions everything from medication, to counseling, dietary control- a whole slew of stuff- so once again times change and so do treatments and diagnoses.
From a gynecologic standpoint or from a hormonal standpoint what goes on is that you have episodes or periods of high amounts of hormonal fluctuations- and this goes back to one of the less understood characteristics of estrogen where it acts almost a neuroprotective type hormone. It’s soothing to the neurons to the activity that’s going on there and so in times when estrogen levels vary wildly you can see manifestations or exacerbations of this condition so during puberty, postpartum and menopause are the three main times in an ovary-owning person’s life when they may notice exacerbations of the symptoms.
With puberty, you have big ups and downs- obviously postpartum with pregnancy you’ve had very high levels of estrogens and the body and then they collapse and then with menopause obviously things are taking a downward term too. Those low levels of estrogen make the neurons act more friable and erratic and so you have more prevalence of the symptoms where patients feel like they can’t concentrate, they can’t remember things, they have brain fog, they feel like they can’t sit still, they don’t rest well at night, etc…
Patients with ADHD in general have intrinsic dopamine which is a neurotransmitter that produces less endogenous dopamine being produced and so what that means is that the patient has to get those dopamine hits from external stimuli, so instead of being able to say, “oh this is really interesting I’m going to keep focused” instead it, “this is now starting to get boring oh look that’s a pretty light oh that’s a squirrel!” whatever it may be.
From a hormonal standpoint testosterone has dopaminergic effects and so testosterone levels go up. Those intrinsic dopamine levels may be kind of higher or those dopamine receptors are getting plugged more well once again in these periods of hormonal fluctuation or hormonal decline testosterone is going to be going down as well because remember the ovaries are the primary producers of testosterone in the body and so if gonadal function starts to decline then you will see those testosterone levels start to go down too.
So what does this mean in terms of sexual functioning?
Well we know that patients with ADHD a lot of times have a higher rate of sexual issues typically you may see that patients have a harder time with arousal and then with orgasm as well if you have a hard time kind of staying focused while you are doing sexual acts, you may find that you lose a little bit of enjoyment with them that you have a hard time maintaining that aroused state. You may find that you have a hard time achieving orgasm as well. A Common treatment for orgasmic dysfunction in this case is the use of medications for ADHD. Adderall is is documented for that. We also sometimes use Concerta or Ritalin, but basically the thought is that the patient then can focus more on what’s going on at hand and so then they have an easier time achieving that level of sexual satisfaction that they want to see from a hormonal standpoint
If you have a a higher rate of ADHD because of lower testosterone levels replacing testosterone may actually help not only with sexual function there but also the ADHD type symptoms.
I’m not saying that everyone who has ADHD needs to be on testosterone but it’s something to consider if you have both of those issues – your sex drive is lower and you deal with ADHD.
Hey everyone, it’s Friday, which means it’s time for our weekly compilation video. As you can see, my office is getting cleaned out here in Bartlesville as I transition over to The Haven Center for Sexual Medicine and Vulvo Vaginal Disorders. The clinic opens on the 4th of October, so if you have any questions about that, be sure to send them my way.
Next Monday night, Jacqueline from the Lost Labia Chronicles and I are doing an Instagram live discussing lichen sclerosus and autoimmune disease. So, if you’re watching this today and have questions about that, shoot either her or myself a message, and we’ll answer them.
This week, we’ve been talking about Ehlers-Danlos Syndrome (EDS) and how it relates to women’s health. If you’re unfamiliar with EDS, it’s essentially a collection of syndromes or conditions that affect the way connective tissue forms. While many think of collagen in terms of skin, it’s present throughout the body in joints, muscles, and blood vessels. Therefore, any condition affecting collagen can lead to various issues.
Currently, there are 13 described EDS subtypes, but there could be more. Each subtype presents unique challenges, so seeking a healthcare provider knowledgeable in the condition is crucial for proper treatment.
In gynecology, EDS primarily impacts pregnancy, pelvic health, sexual health, menstruation, and menopausal changes. Throughout different life stages, patients may experience specific challenges:
Pre-pubertal: Children with EDS, especially hypermobility types, may exhibit flexibility and joint issues. Vigilance is required to identify signs like frequent dislocations or strains.
Menstruation: EDS patients often have heavier periods due to impaired uterine cramping and increased vascular fragility.
Sexual Activity: Pain with penetration and decreased lubrication are common, stemming from fragile skin, tear-prone tissues, and pelvic floor spasms.
Pregnancy: EDS may lead to increased joint pain, preterm labor risk, and complications during childbirth, such as rapid or prolonged labor.
Postpartum: Pelvic organ prolapse and delayed wound healing, including after C-sections, are more prevalent.
Menopause: Genitourinary symptoms of menopause, such as vaginal dryness and pain with intercourse, are exacerbated in EDS patients due to collagen-related issues.
Despite advancements, diagnosing EDS remains challenging, often requiring genetic testing or skin biopsies. However, awareness and understanding among healthcare providers can aid in timely diagnosis and management.
EDS is not just a medical curiosity but a complex condition that profoundly affects patients’ lives. The key takeaway is self-advocacy; if something feels wrong, seek professional help and find providers who understand EDS. Though rare, EDS may be more common than we think, and as our knowledge expands, so will our ability to support those affected.
In conclusion, navigating EDS requires a multidisciplinary approach and ongoing education. By recognizing its impact on women’s health and empowering patients to advocate for themselves, we can strive for better outcomes and improved quality of life. That’s it for today’s video.