Platelet-Rich Plasma (PRP) therapy has garnered significant attention in recent years for its remarkable therapeutic potential across various medical disciplines. From orthopedics to dermatology, PRP’s regenerative properties have revolutionized treatment approaches, offering a natural and effective solution to a wide range of conditions. In this comprehensive guide, we delve into the depths of PRP therapy, unraveling its mechanisms, applications, and the compelling evidence supporting its therapeutic benefits.
Understanding Platelet-Rich Plasma (PRP):
PRP therapy harnesses the body’s innate healing mechanisms by utilizing a concentrated form of platelets derived from the patient’s own blood. Platelets are rich in growth factors and cytokines, bioactive molecules that play pivotal roles in tissue repair, regeneration, and inflammation modulation. By isolating and concentrating these platelets, PRP augments the body’s healing response, accelerating tissue repair and promoting optimal recovery.
Mechanisms of Action:
The therapeutic efficacy of PRP stems from its multifaceted mechanisms of action:
Stimulating Tissue Repair: Platelet-derived growth factors and cytokines promote angiogenesis (formation of new blood vessels) and recruit reparative cells to the site of injury, facilitating tissue regeneration and wound healing.
Modulating Inflammation: PRP exerts anti-inflammatory effects by inhibiting pro-inflammatory cytokines and promoting the secretion of anti-inflammatory mediators, thus reducing inflammation and promoting tissue homeostasis.
Enhancing Collagen Production: Growth factors within PRP, such as platelet-derived growth factor (PDGF) and transforming growth factor-beta (TGF-β), stimulate fibroblast activity and collagen synthesis, contributing to tissue remodeling and improved structural integrity.
Therapeutic Applications of PRP:
Orthopedics and Sports Medicine: PRP has emerged as a promising treatment modality for musculoskeletal injuries, including tendonitis, ligament sprains, and osteoarthritis. Injections of PRP into affected joints or soft tissues promote tissue repair, alleviate pain, and enhance functional outcomes, making it a valuable adjunct to conventional therapies.
Dermatology and Aesthetics: PRP’s regenerative properties have revolutionized dermatological and aesthetic treatments. From hair restoration and facial rejuvenation to scar revision and wound healing, PRP injections or topical applications stimulate collagen production, improve skin texture, and promote hair growth, offering natural and long-lasting results.
Dentistry: In oral and maxillofacial surgery, PRP is used to enhance bone regeneration and promote tissue healing following procedures such as dental implant placement, bone grafting, and periodontal surgery. By accelerating osseointegration and reducing postoperative complications, PRP improves treatment outcomes and patient satisfaction.
Chronic Wound Management: Chronic wounds, such as diabetic ulcers and venous leg ulcers, pose significant challenges to healthcare providers. PRP therapy accelerates wound healing by promoting angiogenesis, tissue granulation, and epithelialization, thereby reducing healing time and preventing complications.
Ophthalmology: In ophthalmic surgery, particularly in procedures such as corneal transplantation and refractive surgery, PRP eye drops or subconjunctival injections facilitate corneal wound healing, reduce inflammation, and minimize postoperative complications, leading to improved visual outcomes.
Clinical Evidence and Research Findings:
The therapeutic benefits of PRP are supported by a robust body of scientific evidence and clinical studies. Meta-analyses and systematic reviews have consistently demonstrated the efficacy of PRP across various medical specialties, confirming its safety, efficacy, and potential as a cost-effective treatment option.
For instance, a meta-analysis published in the Journal of Orthopaedic Surgery and Research concluded that PRP injections significantly improved pain and functional outcomes in patients with knee osteoarthritis compared to placebo or conventional therapies. Similarly, a systematic review in the Journal of Dermatological Treatment found that PRP therapy yielded positive results in promoting hair growth and improving hair density in patients with androgenetic alopecia.
Safety Considerations and Future Directions:
PRP therapy is generally considered safe, with minimal risk of adverse effects, owing to its autologous nature. However, as with any medical procedure, appropriate patient selection, proper technique, and adherence to established protocols are essential to ensure optimal outcomes and minimize potential risks.
Looking ahead, ongoing research efforts aim to further elucidate the underlying mechanisms of PRP therapy, optimize treatment protocols, and explore novel applications across diverse medical disciplines. With continued advancements in biotechnology and regenerative medicine, PRP holds immense promise as a versatile and potent therapeutic tool, empowering healthcare providers to deliver personalized and holistic care to patients worldwide.
Platelet-Rich Plasma (PRP) therapy represents a paradigm shift in regenerative medicine, offering a natural and effective solution to a myriad of medical conditions. From orthopedic injuries to dermatological concerns, its regenerative properties hold the key to accelerated healing, improved functional outcomes, and enhanced quality of life for patients. As research continues to unveil its therapeutic potentials and clinical applications, PRP stands poised to revolutionize healthcare, ushering in a new era of personalized and regenerative therapies.
In the realm of holistic healthcare, innovative approaches continuously emerge to address diverse wellness needs. Among these, Celluma Light Therapy stands out as a promising modality that harnesses the power of light to stimulate healing and promote overall well-being. From skincare to pain management, its versatile applications have garnered attention from both practitioners and individuals seeking natural and non-invasive solutions. Let’s delve into the depths of Celluma Light Therapy, exploring its benefits and therapeutic effects.
Unveiling Celluma Light Therapy:
Celluma Light Therapy represents a fusion of cutting-edge technology and ancient healing principles. At its core lies the principle of photobiomodulation, a process wherein specific wavelengths of light interact with cellular structures to trigger biochemical reactions. Developed by NASA to accelerate wound healing and tissue regeneration in space, this technology has transcended its aerospace origins to revolutionize healthcare on Earth.
How Celluma Light Therapy Works:
At the heart of Celluma lies a matrix of light-emitting diodes (LEDs) that emit specific wavelengths of light, including blue, red, and near-infrared. Each wavelength penetrates the skin at varying depths, targeting different cellular processes.
Blue Light (415nm): With its antibacterial properties, blue light targets the acne-causing bacteria, effectively reducing breakouts and inflammation.
Red Light (630nm): Penetrating deeper into the skin, red light stimulates cellular activity, promoting collagen production, and enhancing tissue repair. It’s instrumental in skin rejuvenation, wrinkle reduction, and wound healing.
Near-Infrared Light (830nm): Known for its profound tissue penetration, near-infrared light facilitates pain relief, reduces inflammation, and accelerates healing processes.
The Benefits:
Skin Rejuvenation: Celluma Light Therapy offers a non-invasive alternative to traditional skincare treatments. By stimulating collagen production and improving cellular function, it diminishes fine lines, wrinkles, and age spots, resulting in a more youthful complexion.
Acne Treatment: Acne, a common dermatological concern, often stems from bacterial overgrowth and inflammation. By targeting the underlying causes, Celluma effectively combats acne, reducing both the frequency and severity of breakouts.
Pain Management: Chronic pain can significantly impair one’s quality of life. Celluma’s near-infrared light penetrates deep into tissues, providing relief from musculoskeletal pain, arthritis, and inflammation, without the side effects associated with medications.
Wound Healing: Whether it’s a surgical incision, a sports injury, or a minor cut, wound healing can be accelerated with Celluma Light Therapy. By enhancing circulation and cellular repair mechanisms, it promotes faster recovery and minimizes scarring.
Mood Enhancement: Light therapy isn’t just beneficial for the body; it also uplifts the spirit. The gentle warmth of Celluma’s light can have mood-enhancing effects, combating seasonal affective disorder (SAD) and promoting relaxation and well-being.
for hair regrowth
for acne treatment
for reducing fine lines
Clinical Evidence:
The efficacy of Celluma Light Therapy is supported by a growing body of scientific research. Clinical studies have demonstrated its effectiveness in various applications, from skincare to pain management. Notably, a study published in the Journal of Clinical and Aesthetic Dermatology found that LED therapy, including Celluma, significantly improved acne severity and skin texture after just four weeks of treatment.
Incorporating Celluma into Your Wellness Routine
Integrating Celluma Light Therapy into your wellness routine is simple and convenient. Whether you visit a professional spa or invest in a personal device for home use, regular sessions can yield significant benefits. Treatments are painless, non-invasive, and require minimal downtime, making them suitable for individuals of all ages and skin types.
In the pursuit of holistic health and wellness, Celluma Light Therapy shines as a beacon of innovation and efficacy. By harnessing the power of light, it offers a gentle yet potent approach to skincare, pain management, and overall rejuvenation. As research continues to unveil its therapeutic potentials, Celluma stands poised to illuminate the path toward optimal well-being, one radiant session at a time.
In a world where natural solutions are increasingly sought after, Celluma Light Therapy emerges as a beacon of hope, offering a gentle yet potent approach to healing and rejuvenation. Whether it’s banishing acne, easing pain, or promoting relaxation, its versatile applications cater to diverse wellness needs, empowering individuals to embrace the light and embark on a journey toward holistic well-being.
Ready to Try Celluma? Contact Haven to schedule a consult and see if Celluma is right for you.
This week, our focus turned to the intricate world of thyroid disease, a topic that impacts millions worldwide yet remains largely misunderstood by many. Delving into the complexities of this glandular dysfunction, we aim to shed light on its various manifestations, diagnostic measures, and treatment modalities.
The thyroid, a butterfly-shaped gland nestled in the neck, orchestrates a symphony of metabolic processes vital for cellular growth and activity. Its importance cannot be overstated, as it governs everything from metabolism to mood regulation. Despite its small size, the thyroid wields considerable influence over our overall well-being.
Thyroid disease encompasses a spectrum of conditions, with hypothyroidism (low thyroid functioning) and Hashimoto’s thyroiditis taking center stage in our discussion. The signs and symptoms of thyroid dysfunction are diverse, ranging from weight fluctuations to mood disturbances. Whether it’s the lethargy of hypothyroidism or the restlessness of hyperthyroidism, the impact on one’s quality of life can be profound.
Diagnosing thyroid disease involves a multifaceted approach, with thyroid hormone levels serving as key indicators. Thyroid-stimulating hormone (TSH), produced by the pituitary gland, acts as a barometer of thyroid activity. Elevated TSH levels often signify hypothyroidism, whereas decreased levels suggest hyperthyroidism. Additionally, assessing thyroid antibodies like thyroid peroxidase (TPO) aids in identifying autoimmune thyroid conditions such as Hashimoto’s disease.
Treatment strategies for thyroid disorders vary depending on the underlying cause and severity of symptoms. Thyroid hormone replacement therapy, utilizing medications like levothyroxine or a combination of T3 and T4 hormones, remains the cornerstone of management. Beyond conventional medications, emerging research underscores the role of adjunctive therapies such as selenium, vitamin D, and certain dietary modifications in optimizing thyroid function.
Moreover, thyroid disease intersects with various aspects of reproductive health, underscoring its relevance in gynecological and fertility contexts. Conditions like polycystic ovarian syndrome (PCOS) and primary ovarian insufficiency often coexist with thyroid dysfunction, highlighting the intricate interplay between endocrine systems.
For individuals grappling with thyroid nodules or concerns about thyroid cancer, vigilance is paramount. While thyroid cancer typically progresses slowly and responds well to treatment, early detection through regular screenings and prompt medical evaluation is essential.
In conclusion, navigating the landscape of thyroid disease requires a nuanced understanding of its complexities. As healthcare providers, we must remain vigilant in recognizing its myriad presentations and empowering patients with the knowledge to advocate for their thyroid health. By fostering collaboration between patients, clinicians, and specialists, we can strive towards improved outcomes and enhanced quality of life for all affected by thyroid disorders.
In our modern world, conversations about sexual health and wellness are increasingly prevalent, yet some aspects remain shrouded in misunderstanding or silence. One such topic is arousal disorders, a complex array of conditions that can profoundly impact an individual’s sexual experiences and relationships.
In a recent YouTube video, Dr. Babb, a renowned expert in sexual medicine, delved into the nuances of arousal disorders, focusing particularly on the physiological and psychological aspects that contribute to these conditions. Throughout the discussion, Dr. Babb emphasized the importance of distinguishing arousal from desire, highlighting how they are distinct yet interconnected components of human sexuality.
Desire, as Dr. Babb explained, stems from the mind—a complex interplay of neurotransmitters and psychological factors that drive one’s interest in sexual activity. Arousal, on the other hand, is the physiological response to that desire, involving changes in heart rate, breathing, blood flow, and genital response. These two components must align for optimal sexual functioning, but when they diverge, individuals may experience frustration, confusion, or distress.
One notable condition discussed by Dr. Babb is Persistent Genital Arousal Disorder (PGAD), now known as Genitopelvic Dysesthesia. While not the focus of the video, PGAD warrants its own in-depth exploration due to its unique challenges and complexities.
From a physiological standpoint, arousal is mediated by the parasympathetic nervous system, signaling safety and relaxation. Conversely, orgasm is mediated by the sympathetic nervous system, often associated with the fight-or-flight response. Achieving full arousal requires a sense of comfort and safety, factors that can be disrupted by various medical conditions, medications, or psychological issues.
Dr. Babb elaborated on the myriad factors that can interfere with arousal, including hypertension, diabetes, nerve damage, and trauma. Addressing these underlying causes may involve medication, therapy, or lifestyle modifications tailored to each individual’s needs. For example, medications like sildenafil can enhance blood flow to genital tissues, while therapies such as pelvic floor exercises or guided masturbation may help address psychological barriers to arousal.
Moreover, Dr. Babb underscored the importance of considering neurodivergent conditions like ADHD, which can affect attention and focus during sexual experiences. By recognizing and addressing these factors, individuals and healthcare providers can work collaboratively to develop holistic treatment plans that address both physical and psychological aspects of arousal disorders.
In conclusion, Dr. Babb emphasized the prevalence of arousal disorders and the need for compassionate, comprehensive care for affected individuals. By fostering open dialogue, raising awareness, and providing accessible resources, we can support those navigating the complex landscape of sexual health and wellness.
As we continue to expand our understanding of arousal disorders, may we approach these discussions with empathy, respect, and a commitment to promoting sexual well-being for all.
Bringing a new life into the world is an extraordinary journey, but it’s also one that comes with a myriad of physical and emotional changes for the mother. As we delve into the intricacies of postpartum life, it becomes evident that understanding and addressing these changes is crucial for a smooth transition into motherhood.
This week, our discussions revolved around postpartum particularities, covering a spectrum of topics from hormonal fluctuations to pelvic health and sexual wellness. It’s imperative to recognize that the postpartum period extends far beyond the immediate weeks following childbirth, encompassing a significant portion of the first year post-delivery.
Let’s begin by exploring the hormonal changes that accompany pregnancy and childbirth. During pregnancy, there’s a surge in sex hormones, including estrogen, progesterone, and testosterone. However, after delivery, especially for breastfeeding mothers, these hormone levels plummet, often leading to postpartum depression, anxiety, and physiological changes such as vaginal dryness.
Thyroid function is another aspect to consider, as pregnancy can alter thyroid hormone levels, potentially leading to postpartum thyroiditis or even thyroid disorders. Additionally, gestational diabetes can progress to type 2 diabetes post-delivery, highlighting the importance of postpartum health monitoring.
Pelvic health emerges as a focal point in postpartum care, with the pelvic floor bearing significant strain during pregnancy and childbirth. Issues like pelvic organ prolapse, urinary incontinence, and bowel dysfunction can arise, necessitating specialized attention and treatment.
Pelvic floor physical therapy stands out as a gold standard treatment, offering targeted interventions to address pelvic floor dysfunction comprehensively. For those experiencing painful intercourse, whether due to hormonal changes or pelvic floor issues, it’s essential to prioritize comfort and communication with your partner, emphasizing consent and mutual understanding.
Navigating postpartum challenges requires a multidimensional approach, encompassing physical therapy, medical intervention, and open communication with healthcare providers and partners. It’s crucial for new mothers to prioritize self-care and seek support when needed, whether it’s addressing postpartum mood disorders or managing pelvic health concerns.
As we continue to explore the intricacies of postpartum care, let’s foster a culture of understanding and support for mothers navigating this transformative journey. Remember, every postpartum experience is unique, and there’s no one-size-fits-all solution. By advocating for comprehensive postpartum care and fostering open dialogue, we can empower mothers to embrace their postpartum journey with confidence and resilience.
In a world where misinformation often spreads faster than truth, it’s refreshing to delve into the depths of scientific data to uncover the realities of hormone therapy and its relationship with cancer. In a recent video transcript, Dr. Babb embarks on a journey through the complexities of hormone therapy, debunking myths and shedding light on the nuanced realities that underpin this crucial aspect of medical treatment.
Diverse Linguistic Exploration
Before delving into the medical intricacies, Dr. Babb sets the stage by highlighting the linguistic diversity of our world. From Lingala in the Congo to Esperanto, the first constructed international language, and Quiche, a native Incan language found in Peru, the global tapestry of languages mirrors the multifaceted nature of medical science itself.
Navigating Hormone Therapy
Central to Dr. Babb ‘s discourse is the exploration of hormone therapy, particularly its association with cancer treatment. With a focus on gynecologic hormonal symptoms like those associated with menopause, Dr. [Name] emphasizes the importance of education and empowerment in making informed medical decisions.
Drawing from the North American Menopause Society’s consensus statement on hormone therapy, Dr. Babb elucidates the wealth of data available to guide practitioners and patients alike. By dispelling the myth that hormone therapy universally leads to adverse outcomes, Dr. Babb highlights the nuanced considerations that inform treatment decisions.
Unveiling the Breast Cancer Conundrum
A pivotal moment in Dr. Babb’s discourse is the exploration of the Women’s Health Initiative study and its implications for breast cancer treatment. By dissecting the study’s findings, Dr. [Name] elucidates the subtle nuances often overlooked in media narratives. While the study initially sparked fears surrounding hormone therapy and breast cancer, deeper analysis reveals a more nuanced reality.
Embracing Individualized Care
Throughout the discussion, Dr. Babb underscores the importance of individualized care. From considerations of receptor positivity in breast cancer to the nuanced approach required for different cancer types, Dr. Babb advocates for a personalized approach that balances symptom relief with risk mitigation.
Empowering Patients
Perhaps the most poignant message echoed throughout Dr. Babb ‘s discourse is one of empowerment. By encouraging patients to engage in open dialogue with knowledgeable providers, Dr. [Name] empowers individuals to take control of their health journey. Through education and advocacy, patients can navigate the complexities of hormone therapy with confidence, dispelling fears and embracing the potential for improved quality of life.
In conclusion, Dr. Babb’s exploration of hormone therapy serves as a beacon of clarity in a landscape often clouded by misinformation. By embracing science over fear, patients and practitioners alike can forge a path towards informed decision-making and empowered health outcomes.
Last week, we delved into the intricate topic of pudendal neuralgia and potential neuropathy, aiming to unravel the complexities surrounding these conditions. Let’s consolidate our knowledge and explore this subject further.
Firstly, let’s clarify some terminology. Throughout this discussion, I may use the terms “neuralgia” and “neuropathy” interchangeably. Essentially, both refer to either pain with or a disorder of the nerve. “Neuralgia” denotes pain, while “neuropathy” is derived from “pathos,” indicating a disease or condition affecting the nerve.
So, what exactly is potential neuropathy? It involves inflammation or irritation of the pudendal nerve. Originating from the sacrum, specifically the second, third, and fourth sacral nerves, the pudendal nerve travels through the pelvis and branches into three divisions: one leading to the labia and clitoris, another to the perineum, and the third to the anus.
Symptoms of potential neuropathy can range from mild itching to sharp, electric shock-like pain along the course of the nerve. Activities such as prolonged sitting or sexual activity may exacerbate these symptoms. Notably, chronic vulvar itching, especially in the absence of visible skin changes or infections, could indicate potential neuropathy and warrants further investigation.
Various factors can contribute to nerve irritation, including pelvic floor dysfunction, pregnancy, childbirth, pelvic surgeries, and chronic pelvic pain conditions. Additionally, activities like cycling or spinal trauma can also play a role.
Diagnosis involves identifying the location of nerve dysfunction to tailor treatment effectively. Pelvic floor physical therapy is often recommended, focusing on muscle relaxation and strengthening. Intravaginal muscle relaxants or nerve blocks may provide relief, particularly for muscle-related pain.
For patients with spinal issues, consultation with a physical therapist or spine surgeon may be beneficial. Medications such as gabapentin, pregabalin, or amitriptyline can help alleviate nerve pain, alongside adjunctive therapies like low-dose naltrexone.
In certain cases, patients with connective tissue disorders like Ehlers-Danlos syndrome may be predisposed to potential neuropathy, warranting specialized care.
Treatment approaches may vary, ranging from conservative measures to invasive procedures, depending on individual circumstances. If you’re experiencing symptoms of potential neuropathy, don’t hesitate to seek professional assistance and embark on a healthcare journey towards optimal well-being.
Remember, understanding the intricacies of potential neuropathy empowers you to make informed decisions about your health. Together, let’s navigate this journey and strive for a better quality of life.
This week, our discussions have delved into the intricacies of hormonal vestibulitis, exploring various aspects such as diagnosis, treatment, and its correlation with other medical conditions. Before we proceed, let’s take care of some housekeeping matters. Throughout the week, we’ve explored the languages of Banks, Korean, and Georgian, which have sparked some interesting conversations. If you enjoy these diversions, let me know your thoughts. On another note, I appreciate the responses to our query about what “Haven” means to you; your input will shape our upcoming reveal on Monday.
Now, let’s dive into the anatomy and physiology of the vestibule. Anatomically, the vestibule represents a specific area of the external genitalia, situated between the labia majora and the hymenal remnant or ring. This region, rich in estrogen and androgen receptors, can manifest symptoms such as irritation, redness, and discomfort when hormone levels are imbalanced.
One of the primary causes of hormonal vestibulitis, particularly in reproductive-age individuals, is the use of oral contraceptive pills (OCPs). Estrogen-containing OCPs, combined with certain progestins, can disrupt hormone levels, leading to vestibular symptoms. Switching to transdermal applications may mitigate these effects to some extent.
Additionally, periods of low estrogen, such as menopause or postpartum stages, can contribute to hormonal vestibulitis. In postmenopausal patients, the decline in ovarian hormone production underscores the importance of considering testosterone supplementation alongside estrogen therapy for optimal symptom management.
Moreover, individuals undergoing treatment for breast cancer, particularly those on aromatase inhibitors, may experience hormonal vestibulitis due to reduced estrogen levels. Collaborating with an oncologist to explore hormone replacement options, such as intravaginal DHEA, can alleviate symptoms while minimizing risks.
Furthermore, autoimmune conditions like lichen sclerosus (LS) can intersect with hormonal vestibulitis. Although LS primarily affects the vulva, individuals with low estrogen levels are at higher risk. While hormonal medications may alleviate vestibular symptoms, steroid therapy remains essential for managing LS and reducing the risk of squamous cell carcinoma.
In conclusion, hormonal vestibulitis underscores the intricate interplay between hormones and vulvar health. Whether caused by medication, physiological changes, or autoimmune conditions, addressing hormonal imbalances is paramount for symptom relief. By understanding these connections, healthcare providers can navigate treatment options effectively, enhancing patient care and quality of life.
In the latest installment of our medical discussion series, we delve into the intricate world of tubal sterilization. Amidst my scratchy voice this week, we’ve explored the nuances of tubal ligations, post tubal ligation syndrome, and the broader landscape surrounding tubal procedures.
This week’s linguistic journey took us through Dutch from the Netherlands, Wattle from a native Aztec language, and Yoruba from Nigeria. But let’s refocus on the medical intricacies of tubal sterilization and how it intersects with recent changes in reproductive rights.
Tubal sterilization, fundamentally, is a form of surgery aimed at preventing pregnancy. Typically performed laparoscopically or through incisions during C-sections or postpartum deliveries, it involves disrupting the fallopian tubes’ function to impede the egg’s journey to meet sperm, thereby averting fertilization.
The surgical techniques vary, from traditional ligation to newer methods like salpingectomy, where the entire tube is removed. However, reversibility and insurance coverage pose significant considerations. Reversal surgeries, though available, are complex and often out-of-pocket expenses, contrasting with the increasing accessibility of in vitro fertilization (IVF).
While tubal sterilization boasts high success rates in preventing unintended pregnancies, it’s not foolproof. Ectopic pregnancies, occurring outside the uterus, remain a potential complication. Moreover, the decision to undergo sterilization should be weighed against the possibility of future reversals and associated challenges.
Enter the enigmatic post tubal ligation syndrome (PTLS), characterized by a constellation of symptoms akin to menopause. Despite lacking definitive medical explanations, theories abound, implicating disruptions in ovarian circulation or hormonal shifts post-surgery.
The landscape surrounding PTLS is contentious, with limited empirical evidence in medical literature. Yet, patient experiences underscore its significance, prompting deeper exploration into its mechanisms and management.
As medical practitioners, our understanding of tubal sterilization’s implications extends beyond surgical techniques. It encompasses nuanced discussions on patient autonomy, reproductive rights, and informed decision-making, especially amidst evolving legal and social landscapes.
In conclusion, tubal sterilization transcends mere surgical interventions; it embodies broader narratives of reproductive health, choice, and empowerment. As we navigate these discussions, let’s ensure inclusivity, empathy, and evidence-based practices, shaping a more informed and compassionate healthcare landscape for all.
Menopause is something that carries with it a multitude of questions and idiosyncrasies. That said, I am going to be focusing on some of the most common concerns hear about menopause, as well as address the most common questions that I receive in the office. I also asked my professional Facebook page members if they had any questions, and will answer those, too.
Part 1: The Basics
Menopause is defined as a year without menstrual periods. Obviously, for women who have had a hysterectomy, or who are on medication that inhibits menstruation, this definition is a little bit more difficult to use, but for the scope of this blog, that’s what we’re going to go with (as a side note, the FDA defines menopause in those individuals as “six months with an FSH above 40” or “six weeks after removal of the ovaries.”) From an endocrine standpoint, menopause is due to a progressive decline in overall ovarian egg volume. Unlike sperm, which are produced continuously, ovaries contain a set number of eggs, and with hormonal changes such as puberty, menstruation, childbirth, etc., that number begins to drop. As the number of eggs diminish, so do the number of follicles that help produce estrogen (see the previous blog on the menstrual cycle), until the point that the egg cohort is virtually exhausted, and no more follicles are made. No follicles = no periods.
Prior to the actual menopausal transition itself, many people experience multiple months, or even years of “menopausal symptoms.” These symptoms include hot flashes, night sweats, mood swings, sleep disturbances, low libido, weight gain, etc. Honestly, you wouldn’t be too far off to potentially attribute any feeling of overall malaise or just “feeling off” to those menopausal hormonal fluctuations. That said, I am not endorsing “blowing off” symptoms for women who are close to their menopausal transition, and saying “it is just hormones,” but if you do a full work-up and nothing comes back abnormal, menopause may be a culprit.
Overall, it is important to remember that menopause is not disease. I’m going to say that again, menopause is not a disease!!!It is a physiologic representation of aging, and in many cultures is actually lauded and highly anticipated. It is interesting to note that in such cultures, the overall rate of “menopausal medicine” is very low. It seems that there is a definite correlation between our cultural idea of aging and age-related transitions, and the need for medical intervention!
Part 2: Q&A
In this section, I’m going to answer some of the most common questions I hear from patients about menopause, as well as address the questions that I received from my professional Facebook page. As always, what I write is for information only, and is not a substitute for actual medical advice. You should always talk to a qualified healthcare professional about your menopausal concerns, and not just go off what you read on the Internet 😉
Q: How long is this going to last?
A: That’s a great question. Let’s look at a couple of graphics to help answer it
This graphic describes the menopausal transition, or what is otherwise known as the “climacteric period.” As you can see, is not uncommon for some women to experience symptoms – usually things like occasional hot flashes, mood swings, and weight gain – up to eight years prior to the actual onset of menopause itself. About three years or so prior to a final period, a patient becomes perimenopausal, and menstrual irregularities become more common. When a patient stops having menses altogether, the menopause countdown commences. The year after the final menses, one can officially say they are menopausal.
This much more complicated graphic goes into the timeline after that final menses, with early menopause being defined as a time period of four years or less following actual menopause, and late menopause occurring after that until death.
Of the big question with menopause, of course, is how long are the symptoms going to last. The good news is that the vast majority of vasomotor symptoms are time limited, and the majority of people will “outgrow” those symptoms once they are in the late postmenopausal period. Unlike the vasomotor complaints, however, the symptoms of the genitourinary syndrome menopause (GSM) unfortunately do not go away with time, but progressively worsen.
Back to the original question. The answer to “how long is this going to last,” is variable. If we say an average of eight years of menopausal symptoms prior to the actual diagnosis of menopause, and then an average of five years following menopause of postmenopausal symptoms, we’re looking at an average of 13 years. I will also say that there is a very strong racial component to this as well, with people of Asian decent statistically having the shortest duration of bothersome menopausal symptoms (around years), and Black individuals having the longest (average of 10.4 years).
Q: My mother/grandmother/etc. went through menopause early. Am I going to, too?
A: Not necessarily. While roughly 50% to the variations in age at menopause are related to genetic variants, studies have had a hard time demonstrating one specific gene or set of genes that determine age of menopause. As such, hereditary indications such as the age of female relatives when they entered menopause are not good of an indicator as to when any individual woman will go through menopause herself.
Q: What can I do about my symptoms?
A: This is a very complex question. Obviously with any menopausal patient, the first thing to identify is the most bothersome symptom. For some this may be more along the lines of hot flashes/night sweats, for others could be low sex drive and pain with intercourse. Hormone therapy remains the gold standard of treatment for the majority of menopausal symptoms, and has the following FDA approved indications:
Vasomotor symptoms – the above mentioned hot flashes and night sweats
Prevention of bone loss – therapies forosteopenia and osteoporosis
Premature hypoestrogenism – Treatments for women with primary ovarian insufficiency, or who undergo iatrogenic menopause as a result of surgical removal of the ovaries or medication (such as chemotherapy).
Genitourinary symptoms – including vaginal dryness, vulvovaginal atrophy, recurrent urinary tract infections or recurrent vaginal infections, and painful intercourse. This grouping of symptoms is collectively known as the Genitourinary Syndrome of Menopause (GSM).
The past few decades have been monumental in shaping the way we view hormone therapy in the United States. The Woman’s Health Initiative (WHI) is probably the most well-known of the hormonal safety studies, and was instrumental in changing our perspective of hormone therapy as a whole. The data it produced was rather controversial, and ultimately was responsible for a general sense of mistrust about the safety of hormone therapy. Thankfully that position is beginning to shift, as more and more research about “safe” hormone therapies come light. If you want to know more about the WHI, I advise you to check out this link.
As a general rule, when we talk about hormone therapy, we’re talking about the pharmaceutical supplementation of estradiol, progesterone, and/or testosterone. These hormones can be used individually or in conjunction with each other, and have different indications for usage. While there are no hard and fast rules when it comes to the formulation of hormone used (pill, cream, injectable, etc.), there are some basic tenets that need to be followed to make sure that hormone therapy is given safely.
1: For people who have a uterus, any form of systemic estrogen therapy (i.e., pill, patch, cream, injection) needs to be accompanied by either a progesterone or a SERM (selective estrogen reuptake modulator) in order to decrease the chance of endometrial cancer. Local, vaginal estrogen formulations do not require progesterone or SERM therapy.
2: Hormone therapy should be initiated in women younger than 60, or within 10 years of the onset of menopause in order to reduce the overall risk for hormone therapy related adverse events.
3: If possible, FDA-approved formulations of hormone therapy should be used before compounded formulations due to concerns about over/under dosing, lack of safety information, and inadequate efficacy testing. This isn’t to say that there isn’t a place for compounded hormones – I routinely prescribe compounded testosterone because there currently isn’t an FDA-approved formulation of testosterone for women (the discussion of compounded therapies vs. conventional therapies is a whole blog topic on its own), but if an FDA approved formulation exists, it should be tried first.
I would like to take a detour for a second, and talk about testosterone in postmenopausal women. The International Society for the Study of Women’s Sexual Health, in conjunction with the International Society for Sexual Medicine released a position statement on the use of testosterone therapy in women in 2020. This statement, available here, describes the methods in which testosterone can be safely used to improve sexual functioning in postmenopausal women. The gist of the statement is that testosterone can be used to improve symptoms associated with hypoactive sexual desire disorder, but that it needs to be done safely, and testosterone level should be monitored to make sure a woman is not receiving too much testosterone.
Now some people are uncomfortable with the thought of hormone therapy, or may not be a candidate for hormone therapy. For these women, there are other treatments that may be effective to varying degrees. Nonhormonal medications such as Paroxetine or clonidine have been shown to reduce the incidences of vasomotor symptoms, and the newest medication released in the Women’s Health Sphere, Veozah, is a gamechanger when it comes to reduction of both severity and frequency of vasomotor symptoms. In addition to specific medication therapy, increasing dietary intake of calcium and vitamin D may be beneficial in reducing bone loss. For women with genitourinary symptoms, vaginal lubricants and moisturizers can be used both with, and prior to, sexual activity, and may make sex less uncomfortable. I cannot downplay the benefit of environmental and lifestyle changes as well. Menopause experts across the world recommend a healthy diet and adequate exercise, and emotional therapeutics such as cognitive behavioral therapy and hypnotherapy may decrease symptoms, too.
Q: Can you go through menopause because you had a hysterectomy?
A: This is a controversial question. The knee-jerk reaction is no, as a hysterectomy is simply the removal of the uterus, and as we mentioned above, menopause is an expression of ovarian function. That said, I have numerous patients who complain of menopausal symptoms following a hysterectomy, so there has to be some truth to that, right?
I’ve looked through the national library of medicine database, and honestly the data is really quite limited on this phenomenon. Now, I did find a study that looked at removal of the fallopian tubes at the time of hysterectomy, and the development of menopausal symptoms after that procedure. These studies did demonstrate an increased risk of menopausal symptoms within one year following surgery, and from an anatomical standpoint, this makes sense.
I’ve talked previously about the collateral uterine circulation, and how there are vessels that go from the uterus, through the tissue underneath the fallopian tube, to the ovary. Removal of that whole section of tissue (uterus and tube), therefore, would theoretically yield a decrease in ovarian blood flow, which in turn could cause decreased ovarian function. Obviously clinical medicine should never be based off of a single study…but at least there’s a potential explanation as to why some women develop menopausal symptoms following removal of their uterus.
Q: If I start hormone therapy, how long should I stay on it?
A: Honestly, there’s not a definitive answer to this question. Historically, the Beers Criteria was used to determine an “appropriate” length of hormone treatment for women, although recent clinical guidelines have stated that this method is outdated and shouldn’t be followed. The truth of the matter is that long-term hormone use, especially when done correctly, has a very low risk of side effects. That said, every patient needs to have an individualized approach to hormone therapy which includes discussing issues such as desire for length of treatment, benefits versus risks for treatment, as well as ways to discontinue treatment if desired.
I will say that in people with primary ovarian insufficiency (POI), it is recommended that they stay on hormone therapy at least until age 52, which is the median age of menopause in United States.
Q: Does menopause cause other health problems?
A: For most people, the answer to that question is “no.” Now with menopause comes age, and with age comes other health concerns, so you could make the assumption that menopause equals health concerns, but that is really just a causal relationship. We also know that the low-hormone state associated with menopause can increase the risk that a person develops certain health conditions, but once again, it’s not a direct cause. That said, people who go through premature menopause are at a higher than age-related risk for numerous health issues such as osteoporosis, heart disease, cognitive decline, and sexual dysfunction, hence the FDA indication for hormone therapy in women with premature hypoestrogenism.
Q: Is there a good resource for menopause online?
A: Yes! Menopause.org is the website for the North American Menopause Society, and they have a multitude of resources for both patients and providers. They also keep a list of both members of the society, as well as Certified Menopause Practitioners – providers who have undertaken additional training in menopausal medicine, and have passed a national certifying exam.
Well friends, I hope that answered some questions about menopause. As always, if you’d like to discuss your symptoms, including specific therapies and recommendations, please contact our office for a consultation. We’re here to help!



 At the heart of Celluma lies a matrix of light-emitting diodes (LEDs) that emit specific wavelengths of light, including blue, red, and near-infrared. Each wavelength penetrates the skin at varying depths, targeting different cellular processes.
At the heart of Celluma lies a matrix of light-emitting diodes (LEDs) that emit specific wavelengths of light, including blue, red, and near-infrared. Each wavelength penetrates the skin at varying depths, targeting different cellular processes.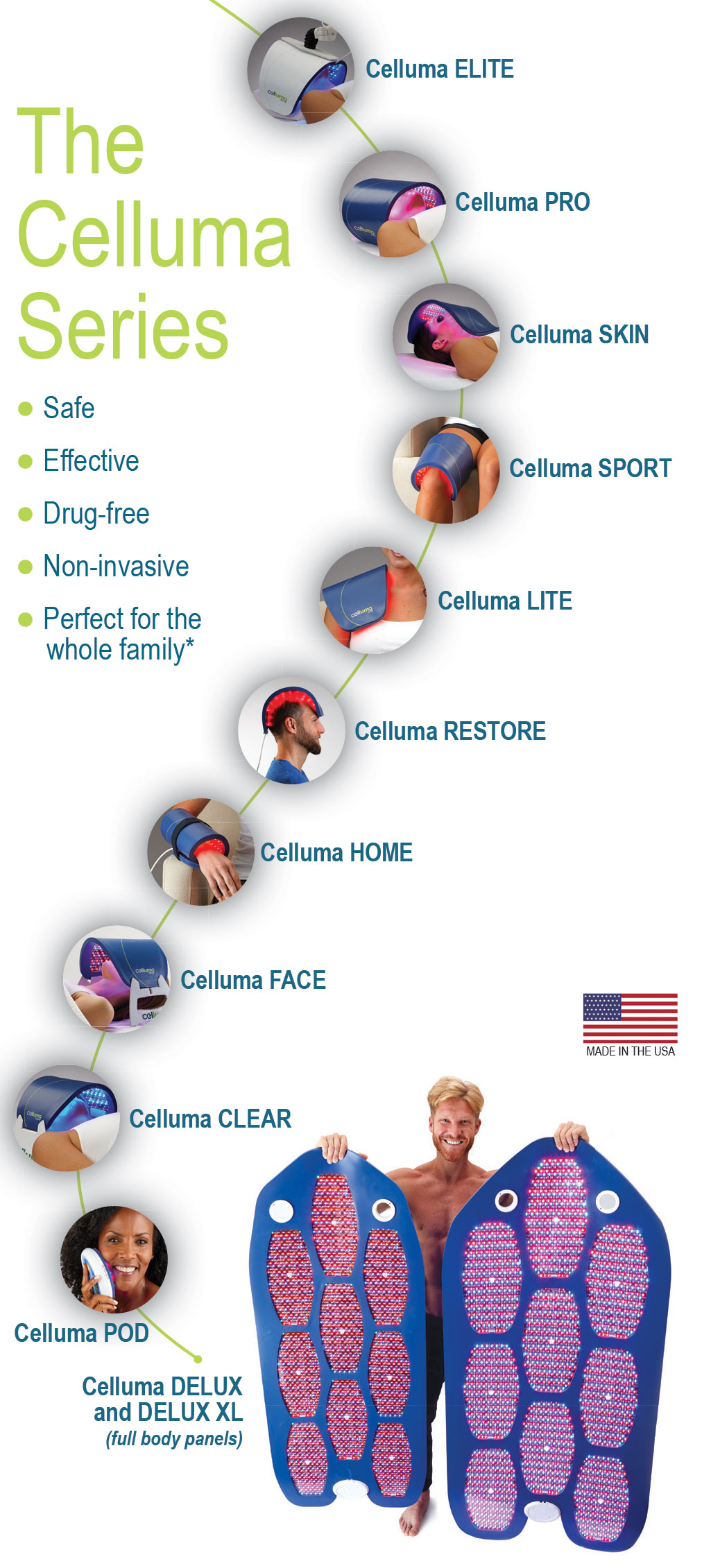 Skin Rejuvenation: Celluma Light Therapy offers a non-invasive alternative to traditional skincare treatments. By stimulating collagen production and improving cellular function, it diminishes fine lines, wrinkles, and age spots, resulting in a more youthful complexion.
Skin Rejuvenation: Celluma Light Therapy offers a non-invasive alternative to traditional skincare treatments. By stimulating collagen production and improving cellular function, it diminishes fine lines, wrinkles, and age spots, resulting in a more youthful complexion.