Have you been feeling fatigued lately? Do you feel your sex drive isn’t as high as it used to be? Are you having hot flushes, night sweats, or feeling irritable? Maybe your hair is falling out, or is it growing in places you wish it wasn’t? Well friends, a hormonal issue may be at the root of your problem. In this blog series we’ll look at the hormonal causes of symptoms such as those listed above, and what to do about them. So without further do, let’s get started!

In this week’s blog, we’re going to be talking about hormonal causes of weight gain, as well as answering some weight-related questions. Before we get started, however, do you realize how big the weight loss industry is? An article in Business Wire in 2019 stated that the weight loss and diet control market in United States was worth around $72 billion – that’s more than the NBA, NHL and MLB combined! From fad diets and over-the-counter weight loss supplements to prescription weight loss medication and bariatric surgery, there’s no doubt that weight loss is a huge moneymaker in the United States. This may not surprise you, however, as a recent study stated that that roughly 70% of Americans are overweight or obese (defined by a BMI of 25 or greater (BMI is a whole other issue, and honestly we shouldn’t be using it for anything, but that’s another blog, too)), and while we’re doing better as a society in terms of promoting a positive body image, if the above numbers mean anything, many of us still would rather be thin (if you’re interested in the “why” behind this, here are some interesting links).
Regardless, the vast majority of people struggle with weight issues at some point in their lives. In terms of unwanted weight gain, multiple factors contribute to this – a decrease in activity level, dietary choices, lifestyle changes, and so on. But what about those people who gain weight even in the face of dieting and exercise? Or, on the other hand, the people that eat anything they want, sit on a couch all day, and are still the same size they were when they were in high school? There’s more to this whole weight gain thing than simply calories in versus calories out, and that, my friends, is what we’re going to talk about today.
Metabolism and Weight
In order to understand weight gain, or weight loss for that matter, you have to understand metabolism. Put simply, metabolism is the rate in which we make, store, and consume energy. People with a high metabolism tend to burn through energy quicker, and the converse is true for people with a lower metabolism. Many things influence metabolism, such as age, health status, or biologic sex. You can find your basal metabolic rate (BMR), i.e. the number of calories you burn throughout the day at rest, utilizing the following formula :
Women: 655 + (4.35 x weight in pounds) + (4.7 x height in inches) – (4.7 x age in years)
Men: 66 + (6.23 x weight in pounds) + (12.7 x height in inches) – (6.8 x age in years)
You can then take that number and multiply it by various modifiers depending on your overall activity level. Here’s a link to an online calculator, in case you don’t want to do the math on your own.
So using this logic, if we calculate our BMR – let’s say it’s 1600 – and we consume less than 1600 calories in a day, we have a caloric deficit. If we’re able to keep this deficit going, we will lose weight. Sounds pretty straightforward…although this isn’t always the case. I can’t even begin to count the number of times I’ve heard “I’ve tried dieting, counting calories, AND exercising, and the weight just doesn’t come off,” or, the even more frustrating statement, “I’ve tried dieting and exercise, and I GAIN weight.” Obviously this is very annoying, not to mention expensive if you’re using any type of subscription weight-loss service. So what do we do next? Well, let’s look at metabolism (and weight gain) from a hormonal perspective, and see how that plays into things.
Metabolism and Hormones
As previously stated, numerous factors influence our metabolism. Hormonally speaking, however, the number of key players are relatively low. Let’s take a quick look at each of them. As a side note, there are many other hormones that influence weight gain, and we’ll get to them a little later.
Insulin: Probably the most important hormone in terms of carbohydrate metabolism, insulin is produced by the pancreas, and affects blood sugar levels. Without getting into too much biochemistry (if you’re in to that, here’s a link), insulin allows glucose (blood sugar) to pass into cells and either be burned for energy, or stored for further use. This is, in essence, a lock and key mechanism. Insulin “unlocks” cells to allow glucose inside, providing those cells with necessary energy. When the cells won’t open for glucose, the glucose is instead stored as fat. This is the main mechanism behind one of the most insidious aspects of weight gain, insulin resistance. Insulin resistance plays a role in multiple conditions, such as diabetes, PCOS, and Metabolic Syndrome, to name a few.
Cortisol: The adrenal glucocorticoid cortisol is the most potent “stress hormone” in our body. It is secreted when our brain perceives we are under stress, be it emotional, physical, or otherwise. Honestly it doesn’t matter if you’re actually under stress or not, if your brain thinks you are, it’s going to tell your adrenal glands to start pumping. From a metabolic standpoint, cortisol activates the sympathetic nervous system (our “fight or flight: response) which causes metabolism to increase, allowing our body to burn through stored energy. In addition, it inhibits the effects of insulin, thereby causing an increase in blood sugar. This is a protective mechanism, as many organs, especially the brain, need glucose to function properly, especially in a high stress situation! Once the stress has resolved, cortisol production decreases, and insulin rises, thereby allowing blood sugar levels to return to normal. In short bursts, this process works wonderfully. With continued, chronic, stress, however (remember, this is perceived stress, too), long-term consequences can arise (see chart below).
Thyroid hormones: The thyroid is in charge of basal metabolic rate. Two main thyroid hormones-thyroxine (T4) and triiodothyronine (T3) are used to increase and decrease metabolic activity as needed throughout the body. T4 is a storage hormone, it is not technically active within cells until an iodine group is removed, and it changes into T3. Let’s look at a diagram…
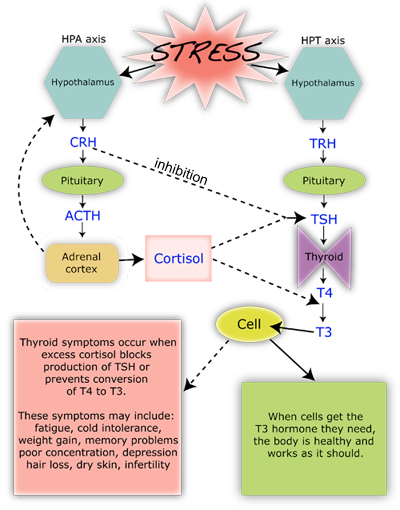
As you can see above, corticotropin releasing hormone (CRH) blocks TSH production, and excess cortisol effects not only TSH, but the conversion of T4 to T3 as well. In other words, chronic stress affects (via cortisol) thyroid hormone production, and in chronically stressed individuals metabolism is decreased.
So What About Weight Loss?
OK, so we’ve talked a lot about metabolism, and looked at the hormones that affect it. So what about weight? Well, while a higher metabolism can lead to weight loss, just because someone has a higher BMR doesn’t mean that they’ll naturally be thin. Weight loss is a very complicated issue, and as we’ve seen above, metabolism is only a small part of the equation.
I asked my Facebook followers if they had any specific questions about weight loss and hormones, and the response was fantastic. I’d like to answer all of them so for the rest of the blog, so I’m going to do more of a Q&A format. I’ll be including links with these questions, so if you’d like more information on a particular topic, check those sites out!
Q: How do I know my weight issues are hormonal in nature?
A: The short answer is that weight gain/loss is, by nature, a hormonal effect. Aside from the above listed hormones that effect metabolism, there are a multitude of other hormones that influence how our body stores energy. Let’s look at a few:
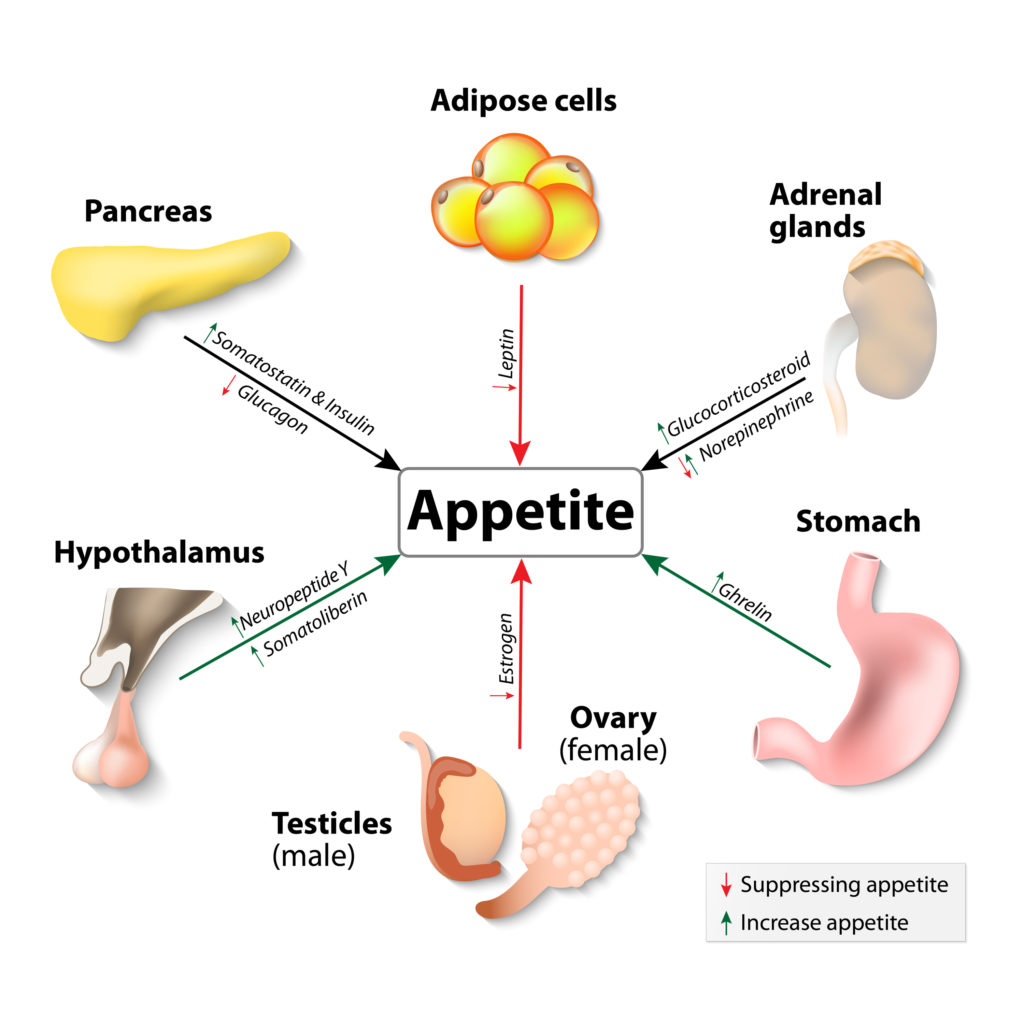
Leptin: Leptin is produced in our fat cells (which means it’s affected by insulin), and is considered a “satiety hormone.” When released, it tells your brain that you have enough fat storage, and therefore helps prevent overeating. Interestingly, obese people tend to have a higher circulating amount of leptin in their blood, which points towards leptin resistance as a possible cause of overeating-related obesity. In addition, leptin is reduced with weight loss, which in essence causes your brain to think you’re starving, which is why it’s so hard to keep the weight off after you lose it!
Ghrelin: In contrast to leptin, ghrelin is a “hunger hormone,” and is produced in the stomach. As you might expect, ghrelin levels are highest right before eating, and drop about an hour after you’ve finished munching. In obese individuals, however, research has demonstrated that ghrelin levels may be abnormally low and that they don’t change as much after eating. This abnormal hormonal behavior is thought to be related to elevated circulating insulin levels, which seem to antagonize ghrelin production.
Estrogens: The estrogen family of hormones plays a role in fat storage and deposition. In times of high estrogen production (puberty, early pregnancy) the body shifts fat cells to subcutaneous areas (namely the hips, breasts, and buttocks) and away from deep, visceral (and abdominal) storage. This relocation of adipose tissue is responsible for the “female form,” and explains why women may lose fullness in those areas after they go through menopause. Increased estrogen intake, be it from birth control pills, hormone therapy, or phytoestrogens (flax, soy) may cause the body to go into a fat-storage mode, contributing to weight gain and obesity.
Peptides: Both Neuropeptide Y (NPY) and Glucagon-Like Peptide-1 (GLP-1) affect our desire to eat. NYP is secreted in times of stress, and stimulates our appetite for carbohydrates (which are rapidly converted into blood sugar). Higher protein intake, as well as prebiotic fiber supplementation may be beneficial in reducing NPY release. GLP-1, on the other hand, is produced in our gut when nutrients enter the intestines, and helps regulate fullness. Chronic inflammation has been shown to reduce GLP-1 production, leading to a decreased since of satiety, which may be a reason so many of us eat when we’re stressed!
Q: Why do some women gain weight after a hysterectomy?
A: This is a very common question. First of all, a hysterectomy is a surgical procedure in which the uterus is removed. A complete hysterectomy involves the removal of the uterus and cervix, and a partial hysterectomy is the removal of the uterus alone-the cervix is left intact. From an anatomic standpoint, the uterus does not produce any substantial level of hormone on its own, but rather has a multitude of hormone receptors. Its removal, therefore, shouldn’t cause any substantial hormonal symptom. So what about post-hysterectomy weight gain? While the reasons for undergoing a hysterectomy are many, most women will have a decrease in activity following surgery. This by itself could lead to some short-term weight gain, but once the “all clear” is given to resume normal activities, that weight should come off. What typically causes hormonal symptoms, however, is when the hysterectomy is accompanied by an oophorectomy, or surgical removal of the ovaries. This puts patients into a iatrogenic, or physician induced, menopause. We’ll discuss menopause in detail in a future blog, but the take-home message is that metabolic activity slows after the menopausal transition and estrogen levels decline, causing a shift in fat distribution as stated above. In addition since endogenous testosterone is also decreased after menopause, muscle mass is lost, and the body’s ability to burn fat and excess calories diminishes.
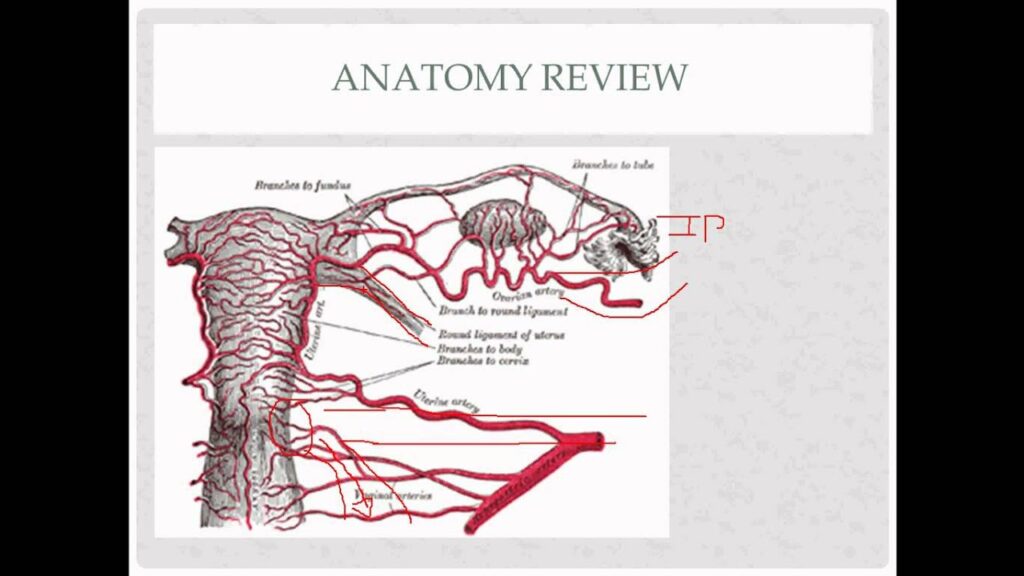
Now I have had patients come in and complain of menopausal symptoms following their hysterectomy, even if the ovaries were left in place. There isn’t really a good medical explanation for this – the research is contradictory. My opinion, however, is when you have multiple patients complaining of the same symptoms following a procedure, there has to be some truth to it. My hypothesis (which is similar to that first study) is as follows: The ovaries received collateral circulation from the vasculature that surrounds the uterus (see picture below). Removal of the uterus can cause a decrease in the blood flow to the ovaries, although not in a substantial enough quantity to cause severe tissue damage. The decrease in blood flow is enough, however, to decrease overall ovarian perfusion, and therefore ovarian function, and decreased ovarian function leads to menopausal symptoms.
Anyone interested in a research study? Let me know!
Q: Can hormones keep me from gaining weight?
A: This is another interesting topic. If you are the type of person that can’t seem to gain weight, no matter what you eat, hormones can definitely play a role. If we rule out obvious hormonal causes such as hyperthyroidism (which boosts metabolic activity), we have to look at those same hunger and fullness hormones listed above. Abnormal levels of Ghrelin and leptin may play a role in people who are chronically thin. Another, albeit not necessarily hormonal cause, would be nutrient malabsorption. Issues with gluten sensitivity, or nutrient and enzymatic deficiency can keep the gut from extracting calories and fats from food, thereby keeping caloric intake low. While this may seem like a “blessing,” nutrient deficiencies and malabsorption actually cause a slew of other symptoms, such as abdominal pain, bloating, as well as diarrhea. If you feel that you are suffering from this condition, I would definitely seek expert care with a gastroenterologist.
Q: Why is a low carb diet good for PCOS?
A: This is an easy one. Many women with polycystic ovarian syndrome also have insulin resistance. In fact, it’s insulin resistance that causes the majority of PCOS symptoms, such as increased facial hair, acne, abnormal bleeding, abdominal weight gain, and oily skin. When insulin levels go up, they suppress Sex Hormone Binding Globulin (SHBG), a regulatory hormone whose sole purpose is to keep free, or unbound, hormones from circulating unchecked. If SHBG is low, then free estradiol and testosterone can run amuck, causing the above stated symptoms. As previously discussed with the insulin paragraph, insulin is responsible for carbohydrate metabolism. Foods that are high in carbohydrates, or more importantly that have a high glycemic index – a measurement of how fast the food is metabolized into glucose – cause a surge in insulin, which over time can lead to insulin resistance. The take-home message for women with PCOS is to try and avoid high glycemic index food. Here’s a list from the American Diabetic Association of foods that have a low glycemic index. We’ll talk more about PCOS in future blogs.
Q: What’s with weight issues and breastfeeding?
A: As to why some women lose weight with breastfeeding, remember that breastfeeding burns an additional 500 or so calories a day. This is because your body is breaking down fat in order to make breastmilk. On the other hand, some women report that they either gain weigh during breastfeeding, or hold onto the weight until they’ve stopped nursing. This is most likely due to either a decrease in activity level, an increase in stress, decrease in sleep, or any combination of the above. In addition, prolactin – the hormone responsible for lactation -causes a down-regulation of estradiol levels. Much like a menopausal woman, a lactating mother will have lower estradiol levels compared to a woman of her same age who is not nursing. This estrogen depletion can cause weight gain as discussed above. I should also state that not eating enough while nursing can lead to weight gain (and a decrease in milk production), as your body goes into “starvation mode,” and holds onto any residual fat stores it has.
Q: Can chronic inflammation lead to weight gain?
A: Of course! Remember cortisol, the body’s most important stress hormone? Well in chronic inflammatory states, our body perceives that inflammation as a stressor, and sends out endogenous corticosteroids to try and reduce it! If you look back up at the graphics, we see that excessive cortisol production not only reduces our ability to utilize insulin effectively, but it also downregulates thyroid function. The end result is more fat deposition, and lowered metabolic activity.
Q: If I’m menopausal (or close to it,) why can’t I lose weight?
A: The menopausal transition brings with it a significant hormonal shift. As a stated above, metabolic activity begins to slow as estrogen and androgen (testosterone) levels naturally decline. A good number of women also report just “feeling worse” during menopause – their sleep quality decreases, they may experience more aches and pains, and they may feel more fatigued, all of which may lower their activity level. This may lead to a multitude of hormonal sequelae, such as:
-Sleep deprivation, which leads to increased stress, which leads to insulin resistance, which leads to weight gain.
-Increased fatigue, which leads to decreased energy, which leads to lowered metabolic activity, which leads to weight gain.
The possibilities go on and on. Keep in mind that as we age our likelihood of developing chronic health conditions rises too, and the diagnosis of something like diabetes mellitus, hypothyroidism, or osteoarthritis can lead to a decrease in activity level as well.
So What Do I Do Now?
Weight loss is a highly controversial, and complex topic, and for me to say something like “let’s just adjust your hormones” downplays how difficult weight loss is. From a medical standpoint, some quicker fixes do exist, such as if someone has insulin resistance, how increasing insulin sensitivity (via diet, medication or supplements) can help shed pounds, or supplementation of thyroid hormone in someone who is hypothyroid. As a general rule though, weight loss is not a simple fix, and in today’s ever increasingly stressful world, it is becoming more difficult to reduce stressors, eat perfectly, and maintain excellent metabolic activity via exercise and supplements.
My advice for those struggling with weight loss is to set realistic goals, and make sure that there isn’t any type of underlying condition hampering your weight loss journey. If you haven’t had a yearly physical, get one – you never know what may turn up. Likewise if there are obvious dietary factors at play (like eating 12 candy bars a day), try and change your diet and see what happens. Additionally, exercise is fantastic, not just for weight loss, but for overall wellbeing and as a stress reliever, and I can’t downplay the importance of a good night sleep, either.
If you’ve done all of those things, and are still struggling with weight loss, you may want to considering seeing a physician who has special training in weight loss therapy. The American Board of Obesity Medicine has a list of physicians who have undergone additional training in the management of weight-related conditions, and is an excellent resource for those patients seeking professional help in their weight-loss journey.
Have a wonderful rest of your day!