How much do you know about your anatomy? What is really considered normal? Should we even say that something is “normal?” Well with this series of blog posts, I hope to dispel some of the myths about female anatomy, as well as discuss certain changes in pelvic anatomy that would warrant a visit to your gynecologist.
As always, this post does not take the place for actual medical advice. If you have concerns or questions, please reach out to your provider. That said, to the vulva!
As always, this post does not take the place for actual medical advice. If you have concerns or questions, please reach out to your provider. That said, to the vulva!
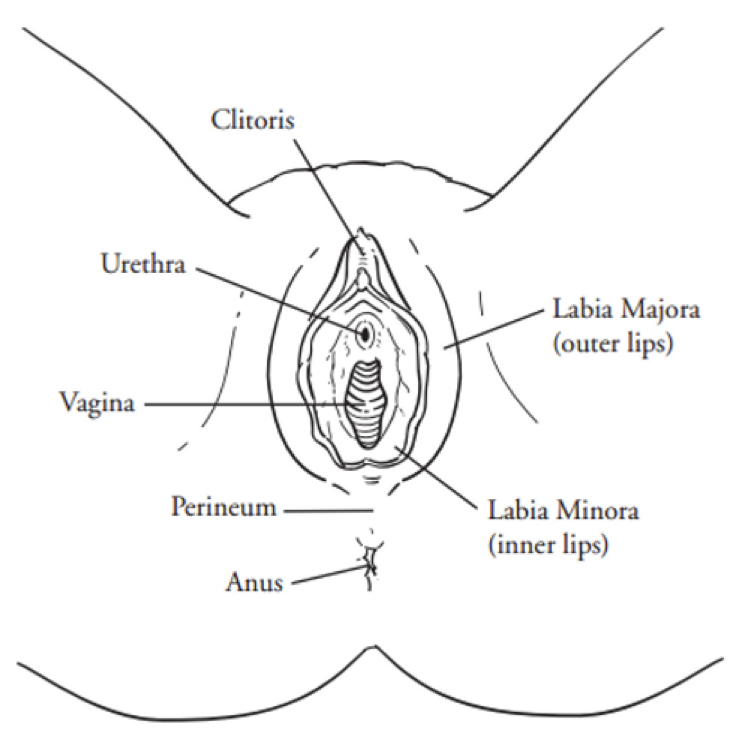
In this week’s blog, I’m going to talk about an oft’ forgotten portion of the vulva, the vestibule, also known as the Vulval Vestibule (archaic term), the Vulvar Vestibule, or the Vestibule of the Vagina. As you can see in the image above, it hasn’t even been marked – which is a travesty, given how important the vestibule is in terms of sexual health. Let’s try again…
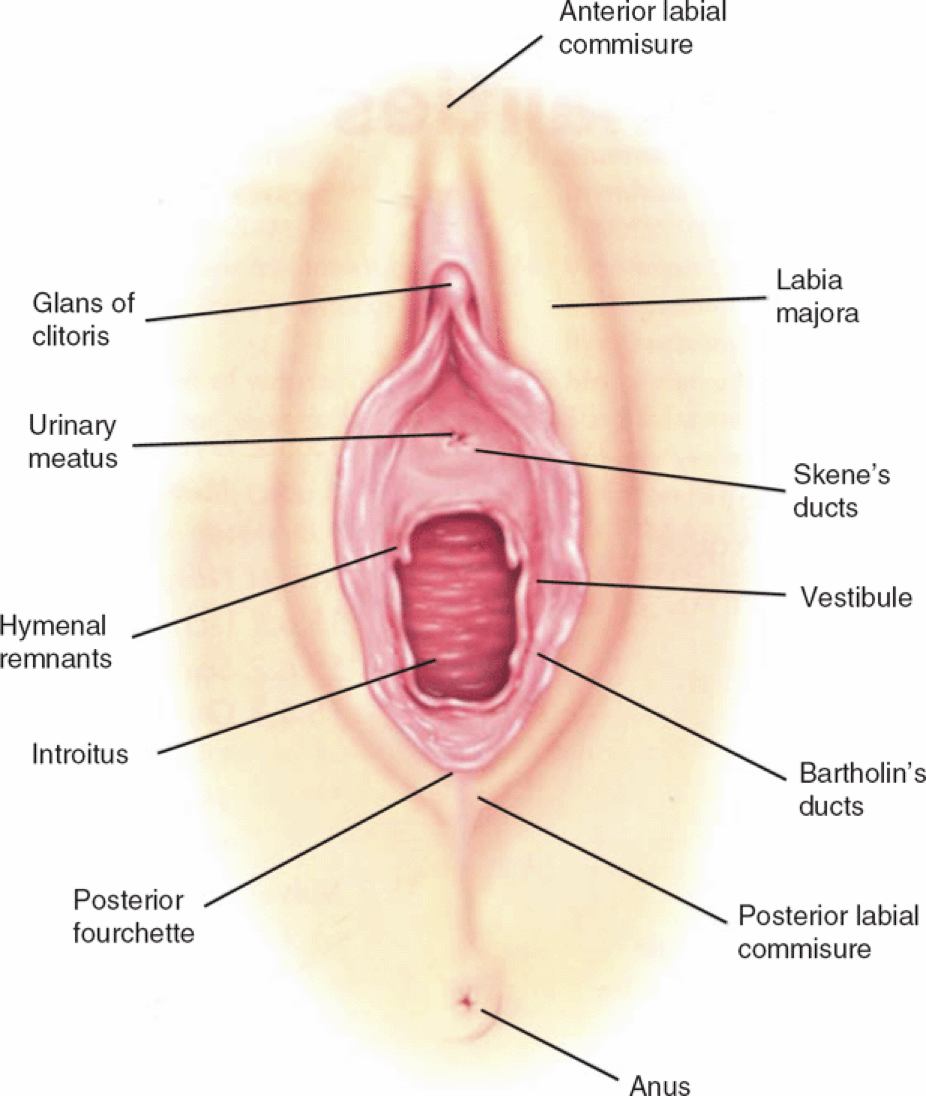
There we go. Much better.
Anatomy
The vestibule is anatomically delineated from Hart’s Line on the labia minora to the Hymenal opening/remnant. It forms from the most distal portion of the urogenital sinus, and as expected, has a male homologue – the prostatic utricle. In addition, the vestibule is the home of the urethra, the paraurethral glands (Skene’s glands), and the Bartholin Glands. It also contains the hymen, the thin membrane that partially covers the opening of the vagina itself.
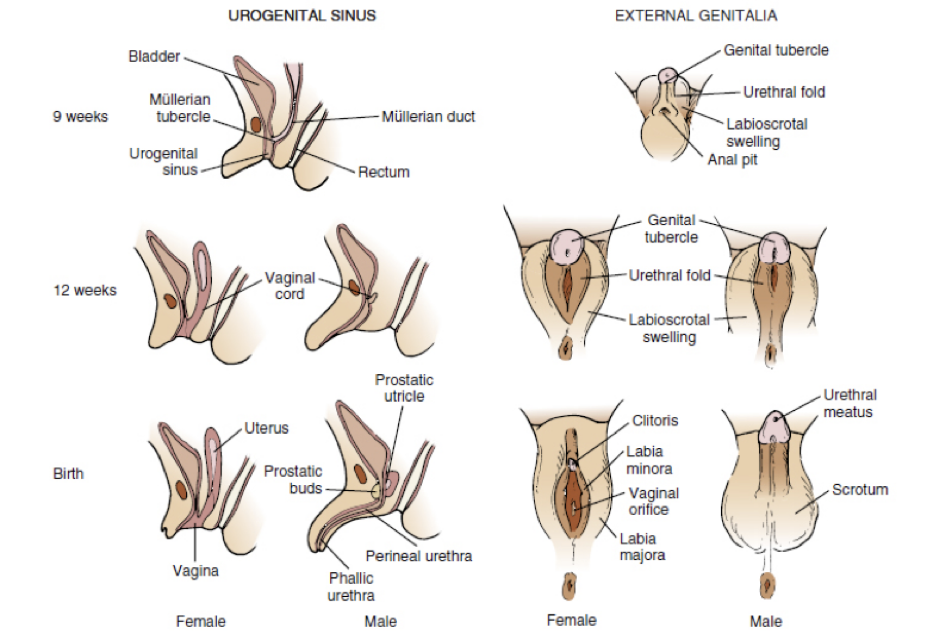
One of the most interesting things about the vestibule is that it is very dense with androgen (testosterone) receptors. This is because both the vestibule, and the prostatic utricle, originate from the same urogenital sinus, an area rich in both androgen and estrogen receptors. As the fetus continues to develop, the vestibule becomes a separate anatomic structure, but due to its origin, it retains its sensitivity to those hormones. Phew! If you’re more of a visual learner, here’s a picture that basically shows that embryologic differentiation.
One of the most interesting things about the vestibule is that it is very dense with androgen (testosterone) receptors. This is because both the vestibule, and the prostatic utricle, originate from the same urogenital sinus, an area rich in both androgen and estrogen receptors. As the fetus continues to develop, the vestibule becomes a separate anatomic structure, but due to its origin, it retains its sensitivity to those hormones. Phew! If you’re more of a visual learner, here’s a picture that basically shows that embryologic differentiation.
Regardless of what type of learner you are, the take home message is this: both estrogens AND androgens are necessary for vestibular health. This is incredibly important when it comes to addressing vestibular complaints. What are some of those complaints, you ask? Well let’s take a look!
Common Vestibular Complaints
Pain: By far, the most common vestibular complaint is pain. The vestibule is rich with nerve endings, and is very sensitive to both pain and pressure. Vestibulodynia, a word that literally translates to “pain in the vestibule,” is the medical terms for…well…pain in the vestibule, and has many potential etiologies, such as bacterial/fungal infection, nerve hyperstimulation, and
hormonal deficiency.
Itching: Vestibular itching is often due to an infectious process. Yeast infections, commonly caused by the fungus Candida albicans, are a very common cause of itching, and often respond quite well to antifungal therapy. That said, while over-the-counter therapy may be a quick and easy way to treat most yeast infections, it doesn’t always work. In my opinion, women with recurrent yeast infections should have a culture taken to determine the exact strand of yeast that is causing the problem, so that the correct antifungal medication can be prescribed. In addition, some women colonize yeast in their rectum, and will have recurrent fungal infections despite vaginal anti-fungal therapy. In this case, a different antifungal – one that is active in the intestine/colon – is needed to help eliminate the problem.
Painful intercourse: Vestibulodynia is often a cause of dyspareunia, or painful intercourse. In my reproductive-age patients, a hormonal vestibulitis – caused by long-term oral contraceptive (OCP) use – is one of the most common causes of painful intercourse I see. A large number of OCPs cause Sex Hormone Binding Globulin (SHBG), a hormone that binds free sex hormones (thyroid hormones, too) to be excreted in high amounts, thereby lowering the amount of available estradiol and testosterone. As stated above, the vestibule requires estradiol and testosterone, and without those sex hormones, it becomes irritated and inflamed, and thus, painful if stimulated. Treatment is based around stopping the oral contraceptive use, as well as correcting those estradiol and testosterone deficiencies.
hormonal deficiency.
Itching: Vestibular itching is often due to an infectious process. Yeast infections, commonly caused by the fungus Candida albicans, are a very common cause of itching, and often respond quite well to antifungal therapy. That said, while over-the-counter therapy may be a quick and easy way to treat most yeast infections, it doesn’t always work. In my opinion, women with recurrent yeast infections should have a culture taken to determine the exact strand of yeast that is causing the problem, so that the correct antifungal medication can be prescribed. In addition, some women colonize yeast in their rectum, and will have recurrent fungal infections despite vaginal anti-fungal therapy. In this case, a different antifungal – one that is active in the intestine/colon – is needed to help eliminate the problem.
Painful intercourse: Vestibulodynia is often a cause of dyspareunia, or painful intercourse. In my reproductive-age patients, a hormonal vestibulitis – caused by long-term oral contraceptive (OCP) use – is one of the most common causes of painful intercourse I see. A large number of OCPs cause Sex Hormone Binding Globulin (SHBG), a hormone that binds free sex hormones (thyroid hormones, too) to be excreted in high amounts, thereby lowering the amount of available estradiol and testosterone. As stated above, the vestibule requires estradiol and testosterone, and without those sex hormones, it becomes irritated and inflamed, and thus, painful if stimulated. Treatment is based around stopping the oral contraceptive use, as well as correcting those estradiol and testosterone deficiencies.
This is by no means an exhaustive list of vestibular complaints. So if you or someone you know has one (or all) of the above symptoms, please reach out! There is soooo much that can be done to improve these conditions. It’s an unfortunate truth that many healthcare providers don’t understand vestibular disease, so expert consultation is important!
Have a wonderful week, and don’t forget – there is hope, there is help, there is Haven Center!
Have a wonderful week, and don’t forget – there is hope, there is help, there is Haven Center!