This week, our focus turned to the intricate world of thyroid disease, a topic that impacts millions worldwide yet remains largely misunderstood by many. Delving into the complexities of this glandular dysfunction, we aim to shed light on its various manifestations, diagnostic measures, and treatment modalities.
The thyroid, a butterfly-shaped gland nestled in the neck, orchestrates a symphony of metabolic processes vital for cellular growth and activity. Its importance cannot be overstated, as it governs everything from metabolism to mood regulation. Despite its small size, the thyroid wields considerable influence over our overall well-being.
Thyroid disease encompasses a spectrum of conditions, with hypothyroidism (low thyroid functioning) and Hashimoto’s thyroiditis taking center stage in our discussion. The signs and symptoms of thyroid dysfunction are diverse, ranging from weight fluctuations to mood disturbances. Whether it’s the lethargy of hypothyroidism or the restlessness of hyperthyroidism, the impact on one’s quality of life can be profound.
Diagnosing thyroid disease involves a multifaceted approach, with thyroid hormone levels serving as key indicators. Thyroid-stimulating hormone (TSH), produced by the pituitary gland, acts as a barometer of thyroid activity. Elevated TSH levels often signify hypothyroidism, whereas decreased levels suggest hyperthyroidism. Additionally, assessing thyroid antibodies like thyroid peroxidase (TPO) aids in identifying autoimmune thyroid conditions such as Hashimoto’s disease.
Treatment strategies for thyroid disorders vary depending on the underlying cause and severity of symptoms. Thyroid hormone replacement therapy, utilizing medications like levothyroxine or a combination of T3 and T4 hormones, remains the cornerstone of management. Beyond conventional medications, emerging research underscores the role of adjunctive therapies such as selenium, vitamin D, and certain dietary modifications in optimizing thyroid function.
Moreover, thyroid disease intersects with various aspects of reproductive health, underscoring its relevance in gynecological and fertility contexts. Conditions like polycystic ovarian syndrome (PCOS) and primary ovarian insufficiency often coexist with thyroid dysfunction, highlighting the intricate interplay between endocrine systems.
For individuals grappling with thyroid nodules or concerns about thyroid cancer, vigilance is paramount. While thyroid cancer typically progresses slowly and responds well to treatment, early detection through regular screenings and prompt medical evaluation is essential.
In conclusion, navigating the landscape of thyroid disease requires a nuanced understanding of its complexities. As healthcare providers, we must remain vigilant in recognizing its myriad presentations and empowering patients with the knowledge to advocate for their thyroid health. By fostering collaboration between patients, clinicians, and specialists, we can strive towards improved outcomes and enhanced quality of life for all affected by thyroid disorders.
Bringing a new life into the world is an extraordinary journey, but it’s also one that comes with a myriad of physical and emotional changes for the mother. As we delve into the intricacies of postpartum life, it becomes evident that understanding and addressing these changes is crucial for a smooth transition into motherhood.
This week, our discussions revolved around postpartum particularities, covering a spectrum of topics from hormonal fluctuations to pelvic health and sexual wellness. It’s imperative to recognize that the postpartum period extends far beyond the immediate weeks following childbirth, encompassing a significant portion of the first year post-delivery.
Let’s begin by exploring the hormonal changes that accompany pregnancy and childbirth. During pregnancy, there’s a surge in sex hormones, including estrogen, progesterone, and testosterone. However, after delivery, especially for breastfeeding mothers, these hormone levels plummet, often leading to postpartum depression, anxiety, and physiological changes such as vaginal dryness.
Thyroid function is another aspect to consider, as pregnancy can alter thyroid hormone levels, potentially leading to postpartum thyroiditis or even thyroid disorders. Additionally, gestational diabetes can progress to type 2 diabetes post-delivery, highlighting the importance of postpartum health monitoring.
Pelvic health emerges as a focal point in postpartum care, with the pelvic floor bearing significant strain during pregnancy and childbirth. Issues like pelvic organ prolapse, urinary incontinence, and bowel dysfunction can arise, necessitating specialized attention and treatment.
Pelvic floor physical therapy stands out as a gold standard treatment, offering targeted interventions to address pelvic floor dysfunction comprehensively. For those experiencing painful intercourse, whether due to hormonal changes or pelvic floor issues, it’s essential to prioritize comfort and communication with your partner, emphasizing consent and mutual understanding.
Navigating postpartum challenges requires a multidimensional approach, encompassing physical therapy, medical intervention, and open communication with healthcare providers and partners. It’s crucial for new mothers to prioritize self-care and seek support when needed, whether it’s addressing postpartum mood disorders or managing pelvic health concerns.
As we continue to explore the intricacies of postpartum care, let’s foster a culture of understanding and support for mothers navigating this transformative journey. Remember, every postpartum experience is unique, and there’s no one-size-fits-all solution. By advocating for comprehensive postpartum care and fostering open dialogue, we can empower mothers to embrace their postpartum journey with confidence and resilience.
This week, our discussions have delved into the intricacies of hormonal vestibulitis, exploring various aspects such as diagnosis, treatment, and its correlation with other medical conditions. Before we proceed, let’s take care of some housekeeping matters. Throughout the week, we’ve explored the languages of Banks, Korean, and Georgian, which have sparked some interesting conversations. If you enjoy these diversions, let me know your thoughts. On another note, I appreciate the responses to our query about what “Haven” means to you; your input will shape our upcoming reveal on Monday.
Now, let’s dive into the anatomy and physiology of the vestibule. Anatomically, the vestibule represents a specific area of the external genitalia, situated between the labia majora and the hymenal remnant or ring. This region, rich in estrogen and androgen receptors, can manifest symptoms such as irritation, redness, and discomfort when hormone levels are imbalanced.
One of the primary causes of hormonal vestibulitis, particularly in reproductive-age individuals, is the use of oral contraceptive pills (OCPs). Estrogen-containing OCPs, combined with certain progestins, can disrupt hormone levels, leading to vestibular symptoms. Switching to transdermal applications may mitigate these effects to some extent.
Additionally, periods of low estrogen, such as menopause or postpartum stages, can contribute to hormonal vestibulitis. In postmenopausal patients, the decline in ovarian hormone production underscores the importance of considering testosterone supplementation alongside estrogen therapy for optimal symptom management.
Moreover, individuals undergoing treatment for breast cancer, particularly those on aromatase inhibitors, may experience hormonal vestibulitis due to reduced estrogen levels. Collaborating with an oncologist to explore hormone replacement options, such as intravaginal DHEA, can alleviate symptoms while minimizing risks.
Furthermore, autoimmune conditions like lichen sclerosus (LS) can intersect with hormonal vestibulitis. Although LS primarily affects the vulva, individuals with low estrogen levels are at higher risk. While hormonal medications may alleviate vestibular symptoms, steroid therapy remains essential for managing LS and reducing the risk of squamous cell carcinoma.
In conclusion, hormonal vestibulitis underscores the intricate interplay between hormones and vulvar health. Whether caused by medication, physiological changes, or autoimmune conditions, addressing hormonal imbalances is paramount for symptom relief. By understanding these connections, healthcare providers can navigate treatment options effectively, enhancing patient care and quality of life.
Menopause is something that carries with it a multitude of questions and idiosyncrasies. That said, I am going to be focusing on some of the most common concerns hear about menopause, as well as address the most common questions that I receive in the office. I also asked my professional Facebook page members if they had any questions, and will answer those, too.
Part 1: The Basics
Menopause is defined as a year without menstrual periods. Obviously, for women who have had a hysterectomy, or who are on medication that inhibits menstruation, this definition is a little bit more difficult to use, but for the scope of this blog, that’s what we’re going to go with (as a side note, the FDA defines menopause in those individuals as “six months with an FSH above 40” or “six weeks after removal of the ovaries.”) From an endocrine standpoint, menopause is due to a progressive decline in overall ovarian egg volume. Unlike sperm, which are produced continuously, ovaries contain a set number of eggs, and with hormonal changes such as puberty, menstruation, childbirth, etc., that number begins to drop. As the number of eggs diminish, so do the number of follicles that help produce estrogen (see the previous blog on the menstrual cycle), until the point that the egg cohort is virtually exhausted, and no more follicles are made. No follicles = no periods.
Prior to the actual menopausal transition itself, many people experience multiple months, or even years of “menopausal symptoms.” These symptoms include hot flashes, night sweats, mood swings, sleep disturbances, low libido, weight gain, etc. Honestly, you wouldn’t be too far off to potentially attribute any feeling of overall malaise or just “feeling off” to those menopausal hormonal fluctuations. That said, I am not endorsing “blowing off” symptoms for women who are close to their menopausal transition, and saying “it is just hormones,” but if you do a full work-up and nothing comes back abnormal, menopause may be a culprit.
Overall, it is important to remember that menopause is not disease. I’m going to say that again, menopause is not a disease!!!It is a physiologic representation of aging, and in many cultures is actually lauded and highly anticipated. It is interesting to note that in such cultures, the overall rate of “menopausal medicine” is very low. It seems that there is a definite correlation between our cultural idea of aging and age-related transitions, and the need for medical intervention!
Part 2: Q&A
In this section, I’m going to answer some of the most common questions I hear from patients about menopause, as well as address the questions that I received from my professional Facebook page. As always, what I write is for information only, and is not a substitute for actual medical advice. You should always talk to a qualified healthcare professional about your menopausal concerns, and not just go off what you read on the Internet 😉
Q: How long is this going to last?
A: That’s a great question. Let’s look at a couple of graphics to help answer it
This graphic describes the menopausal transition, or what is otherwise known as the “climacteric period.” As you can see, is not uncommon for some women to experience symptoms – usually things like occasional hot flashes, mood swings, and weight gain – up to eight years prior to the actual onset of menopause itself. About three years or so prior to a final period, a patient becomes perimenopausal, and menstrual irregularities become more common. When a patient stops having menses altogether, the menopause countdown commences. The year after the final menses, one can officially say they are menopausal.
This much more complicated graphic goes into the timeline after that final menses, with early menopause being defined as a time period of four years or less following actual menopause, and late menopause occurring after that until death.
Of the big question with menopause, of course, is how long are the symptoms going to last. The good news is that the vast majority of vasomotor symptoms are time limited, and the majority of people will “outgrow” those symptoms once they are in the late postmenopausal period. Unlike the vasomotor complaints, however, the symptoms of the genitourinary syndrome menopause (GSM) unfortunately do not go away with time, but progressively worsen.
Back to the original question. The answer to “how long is this going to last,” is variable. If we say an average of eight years of menopausal symptoms prior to the actual diagnosis of menopause, and then an average of five years following menopause of postmenopausal symptoms, we’re looking at an average of 13 years. I will also say that there is a very strong racial component to this as well, with people of Asian decent statistically having the shortest duration of bothersome menopausal symptoms (around years), and Black individuals having the longest (average of 10.4 years).
Q: My mother/grandmother/etc. went through menopause early. Am I going to, too?
A: Not necessarily. While roughly 50% to the variations in age at menopause are related to genetic variants, studies have had a hard time demonstrating one specific gene or set of genes that determine age of menopause. As such, hereditary indications such as the age of female relatives when they entered menopause are not good of an indicator as to when any individual woman will go through menopause herself.
Q: What can I do about my symptoms?
A: This is a very complex question. Obviously with any menopausal patient, the first thing to identify is the most bothersome symptom. For some this may be more along the lines of hot flashes/night sweats, for others could be low sex drive and pain with intercourse. Hormone therapy remains the gold standard of treatment for the majority of menopausal symptoms, and has the following FDA approved indications:
Vasomotor symptoms – the above mentioned hot flashes and night sweats
Prevention of bone loss – therapies forosteopenia and osteoporosis
Premature hypoestrogenism – Treatments for women with primary ovarian insufficiency, or who undergo iatrogenic menopause as a result of surgical removal of the ovaries or medication (such as chemotherapy).
Genitourinary symptoms – including vaginal dryness, vulvovaginal atrophy, recurrent urinary tract infections or recurrent vaginal infections, and painful intercourse. This grouping of symptoms is collectively known as the Genitourinary Syndrome of Menopause (GSM).
The past few decades have been monumental in shaping the way we view hormone therapy in the United States. The Woman’s Health Initiative (WHI) is probably the most well-known of the hormonal safety studies, and was instrumental in changing our perspective of hormone therapy as a whole. The data it produced was rather controversial, and ultimately was responsible for a general sense of mistrust about the safety of hormone therapy. Thankfully that position is beginning to shift, as more and more research about “safe” hormone therapies come light. If you want to know more about the WHI, I advise you to check out this link.
As a general rule, when we talk about hormone therapy, we’re talking about the pharmaceutical supplementation of estradiol, progesterone, and/or testosterone. These hormones can be used individually or in conjunction with each other, and have different indications for usage. While there are no hard and fast rules when it comes to the formulation of hormone used (pill, cream, injectable, etc.), there are some basic tenets that need to be followed to make sure that hormone therapy is given safely.
1: For people who have a uterus, any form of systemic estrogen therapy (i.e., pill, patch, cream, injection) needs to be accompanied by either a progesterone or a SERM (selective estrogen reuptake modulator) in order to decrease the chance of endometrial cancer. Local, vaginal estrogen formulations do not require progesterone or SERM therapy.
2: Hormone therapy should be initiated in women younger than 60, or within 10 years of the onset of menopause in order to reduce the overall risk for hormone therapy related adverse events.
3: If possible, FDA-approved formulations of hormone therapy should be used before compounded formulations due to concerns about over/under dosing, lack of safety information, and inadequate efficacy testing. This isn’t to say that there isn’t a place for compounded hormones – I routinely prescribe compounded testosterone because there currently isn’t an FDA-approved formulation of testosterone for women (the discussion of compounded therapies vs. conventional therapies is a whole blog topic on its own), but if an FDA approved formulation exists, it should be tried first.
I would like to take a detour for a second, and talk about testosterone in postmenopausal women. The International Society for the Study of Women’s Sexual Health, in conjunction with the International Society for Sexual Medicine released a position statement on the use of testosterone therapy in women in 2020. This statement, available here, describes the methods in which testosterone can be safely used to improve sexual functioning in postmenopausal women. The gist of the statement is that testosterone can be used to improve symptoms associated with hypoactive sexual desire disorder, but that it needs to be done safely, and testosterone level should be monitored to make sure a woman is not receiving too much testosterone.
Now some people are uncomfortable with the thought of hormone therapy, or may not be a candidate for hormone therapy. For these women, there are other treatments that may be effective to varying degrees. Nonhormonal medications such as Paroxetine or clonidine have been shown to reduce the incidences of vasomotor symptoms, and the newest medication released in the Women’s Health Sphere, Veozah, is a gamechanger when it comes to reduction of both severity and frequency of vasomotor symptoms. In addition to specific medication therapy, increasing dietary intake of calcium and vitamin D may be beneficial in reducing bone loss. For women with genitourinary symptoms, vaginal lubricants and moisturizers can be used both with, and prior to, sexual activity, and may make sex less uncomfortable. I cannot downplay the benefit of environmental and lifestyle changes as well. Menopause experts across the world recommend a healthy diet and adequate exercise, and emotional therapeutics such as cognitive behavioral therapy and hypnotherapy may decrease symptoms, too.
Q: Can you go through menopause because you had a hysterectomy?
A: This is a controversial question. The knee-jerk reaction is no, as a hysterectomy is simply the removal of the uterus, and as we mentioned above, menopause is an expression of ovarian function. That said, I have numerous patients who complain of menopausal symptoms following a hysterectomy, so there has to be some truth to that, right?
I’ve looked through the national library of medicine database, and honestly the data is really quite limited on this phenomenon. Now, I did find a study that looked at removal of the fallopian tubes at the time of hysterectomy, and the development of menopausal symptoms after that procedure. These studies did demonstrate an increased risk of menopausal symptoms within one year following surgery, and from an anatomical standpoint, this makes sense.
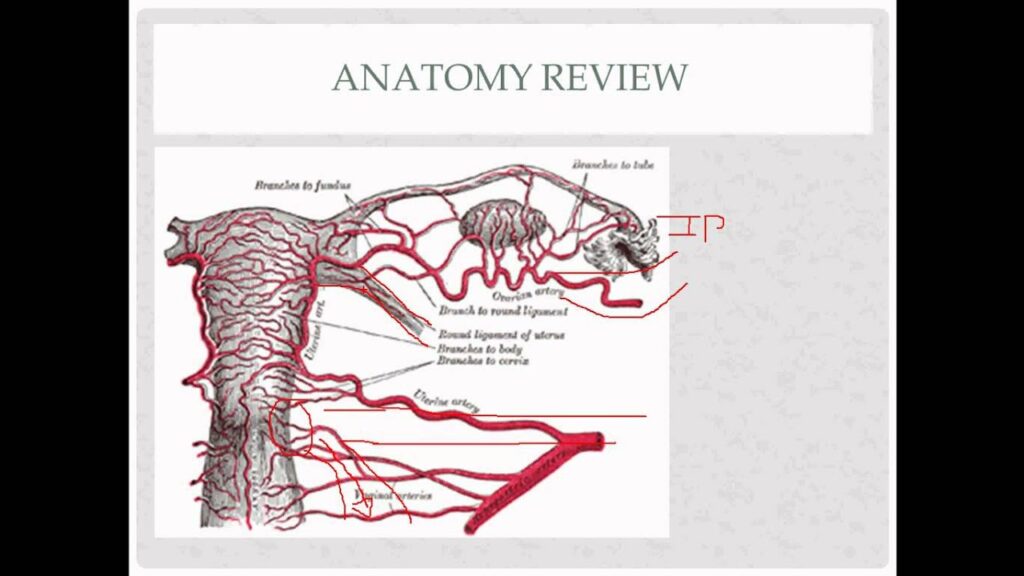
I’ve talked previously about the collateral uterine circulation, and how there are vessels that go from the uterus, through the tissue underneath the fallopian tube, to the ovary. Removal of that whole section of tissue (uterus and tube), therefore, would theoretically yield a decrease in ovarian blood flow, which in turn could cause decreased ovarian function. Obviously clinical medicine should never be based off of a single study…but at least there’s a potential explanation as to why some women develop menopausal symptoms following removal of their uterus.
Q: If I start hormone therapy, how long should I stay on it?
A: Honestly, there’s not a definitive answer to this question. Historically, the Beers Criteria was used to determine an “appropriate” length of hormone treatment for women, although recent clinical guidelines have stated that this method is outdated and shouldn’t be followed. The truth of the matter is that long-term hormone use, especially when done correctly, has a very low risk of side effects. That said, every patient needs to have an individualized approach to hormone therapy which includes discussing issues such as desire for length of treatment, benefits versus risks for treatment, as well as ways to discontinue treatment if desired.
I will say that in people with primary ovarian insufficiency (POI), it is recommended that they stay on hormone therapy at least until age 52, which is the median age of menopause in United States.
Q: Does menopause cause other health problems?
A: For most people, the answer to that question is “no.” Now with menopause comes age, and with age comes other health concerns, so you could make the assumption that menopause equals health concerns, but that is really just a causal relationship. We also know that the low-hormone state associated with menopause can increase the risk that a person develops certain health conditions, but once again, it’s not a direct cause. That said, people who go through premature menopause are at a higher than age-related risk for numerous health issues such as osteoporosis, heart disease, cognitive decline, and sexual dysfunction, hence the FDA indication for hormone therapy in women with premature hypoestrogenism.
Q: Is there a good resource for menopause online?
A: Yes! Menopause.org is the website for the North American Menopause Society, and they have a multitude of resources for both patients and providers. They also keep a list of both members of the society, as well as Certified Menopause Practitioners – providers who have undertaken additional training in menopausal medicine, and have passed a national certifying exam.
Well friends, I hope that answered some questions about menopause. As always, if you’d like to discuss your symptoms, including specific therapies and recommendations, please contact our office for a consultation. We’re here to help!
I recently had a patient visit me for hormonal consultation. For her chief complaint, she listed “my hormones are going crazy.” After some discussion, she revealed that that her hormones were “out of control all the time,” and that they were affecting her quality of life. She stated she had recently been to another provider who told her that “there is no way your hormones could be causing these things – you probably should see a psychiatrist.” Obviously, she did not feel that that advice was very helpful, and after doing some research she had come to the conclusion on her own that, yes, her hormones were causing symptoms.
Our visit was relatively uneventful – she complained of very common symptoms, such as fatigue, weight gain, low sex drive, and an overall sense of “meh.” We talked about potential causes for her symptoms, and I did a physical exam to rule out any obvious anatomic issues (enlarged thyroid, nipple discharge, etc.). We also talked about labs – when, and if, we should order them, and what they might show. In the end, we ended up drawing a fairly standard assortment of laboratory tests, including a blood count, chemistry panel, thyroid profile, and sex hormones. I had her make a return appointment to discuss results, as well as a plan of care.
A few days later we sat in my office, and went over the results. Her complete blood count -totally fine. Comprehensive metabolic panel – no issue. Thyroid panel – negative. Sex hormones – age and cycle appropriate. “How can this be?” She asked. She had the symptoms of a hormonal issue, but the labs provided no answer to her questions. Unfortunately, this is an all too common finding. Even if we look at the labs with a narrower range of “normal,” there are still many times that they do not provide any answer to why someone feels the way they do. In my opinion, this is one reason why we should treat people, and not lab findings, but that’s another blog. That said, it does no good to put someone on, for instance, testosterone replacement if they do not have a testosterone deficiency, so you can’t just treat symptoms without cause.
So now the question becomes “what do we do?” More often than not, the hormonal symptoms that people complain of are not due to some innate, organic dysfunction, but rather a mix of different factors: sleep, stress, diet, etc. Obviously, symptoms require investigation, and it’s the hope of patients and practitioners everywhere that those investigations yield a diagnosis (one that’s treatable, preferably). But more often than not, unfortunately, those queries seem to only yield more questions, such as what to do with labs that are all within normal range, imaging studies that are unremarkable, and so on.
We are left many times without definitive answers in medicine – although we often wish this wasn’t the case. Just as human beings are full color, three-dimensional, complex beings, so too are the things that ail us; disease processes are not simply black and white. When modern medicine fails to give us answers, many of us are left feeling lost. Now, some may turn into alternative, complementary health care practices – clinical nutrition, herbalism, reiki, etc., while others may research even more occult diagnoses, convinced that they are afflicted with conditions that have only affected a small number people. Neither decision would be an incorrect approach – when we’re feeling bad, we often search for answers in a variety of places. I would caution, however, against therapies or treatments that may seem too good to be true. I have seen many ads on the Internet for supplements that “cure all sexual issues,” or for “specialty clinics” that have a 100% success rate in treating symptoms using a proprietary blend of various therapies. Along the same vein, extremely rare medical conditions do exist, but it can be an expensive and frustrating endeavor to rule out every condition that has a symptom of, let’s say, fatigue.
As for our patient from above, in the end we did find a diagnosis, although not one that was necessarily “hormonal.” Further discussion of her sleep habits revealed that she was getting only a few hours of uninterrupted sleep at night. Her husband also divulged that she snored quite a bit, and would also “startle” while she was asleep. A sleep study confirmed the diagnosis of sleep apnea, and I can say that at her last follow-up, she is feeling 100% better thanks to her CPAP.
The take-home message is this. Hormonal symptoms may be from hormonal causes. They may also, however, be from a variety of nonhormonal factors such as sleep deprivation or stress. In the end it behooves the practitioner to look at the patient as a whole, and not just as an organ system or specific symptom. As I’ve said before, people are more than just a collection of vital signs, lab studies, and complaints. A very good friend of mine (who is a family physician) once told me that western medicine is “really good at treating disease, but terrible at treating symptoms.” This is why I feel it is so important to have a good network of non-physician providers (nutritionists, physical therapists, counselors, etc.) who can help when conventional therapy can’t. We’re all in this together, after all.
Have you been feeling fatigued lately? Do you feel your sex drive isn’t as high as it used to be? Are you having hot flushes, night sweats, or feeling irritable? Maybe your hair is falling out, or is it growing in places you wish it wasn’t? Well friends, a hormonal issue may be at the root of your problem. In this blog series we’ll look at the hormonal causes of symptoms such as those listed above, and what to do about them. So without further do, let’s get started!
In this week’s blog, we’re going to be talking about hormonal causes of weight gain, as well as answering some weight-related questions. Before we get started, however, do you realize how big the weight loss industry is? An article in Business Wire in 2019 stated that the weight loss and diet control market in United States was worth around $72 billion – that’s more than the NBA, NHL and MLB combined! From fad diets and over-the-counter weight loss supplements to prescription weight loss medication and bariatric surgery, there’s no doubt that weight loss is a huge moneymaker in the United States. This may not surprise you, however, as a recent study stated that that roughly 70% of Americans are overweight or obese (defined by a BMI of 25 or greater (BMI is a whole other issue, and honestly we shouldn’t be using it for anything, but that’s another blog, too)), and while we’re doing better as a society in terms of promoting a positive body image, if the above numbers mean anything, many of us still would rather be thin (if you’re interested in the “why” behind this, here are some interesting links).
Regardless, the vast majority of people struggle with weight issues at some point in their lives. In terms of unwanted weight gain, multiple factors contribute to this – a decrease in activity level, dietary choices, lifestyle changes, and so on. But what about those people who gain weight even in the face of dieting and exercise? Or, on the other hand, the people that eat anything they want, sit on a couch all day, and are still the same size they were when they were in high school? There’s more to this whole weight gain thing than simply calories in versus calories out, and that, my friends, is what we’re going to talk about today.
Metabolism and Weight
In order to understand weight gain, or weight loss for that matter, you have to understand metabolism. Put simply, metabolism is the rate in which we make, store, and consume energy. People with a high metabolism tend to burn through energy quicker, and the converse is true for people with a lower metabolism. Many things influence metabolism, such as age, health status, or biologic sex. You can find your basal metabolic rate (BMR), i.e. the number of calories you burn throughout the day at rest, utilizing the following formula :
Women: 655 + (4.35 x weight in pounds) + (4.7 x height in inches) – (4.7 x age in years)
Men: 66 + (6.23 x weight in pounds) + (12.7 x height in inches) – (6.8 x age in years)
You can then take that number and multiply it by various modifiers depending on your overall activity level. Here’s a link to an online calculator, in case you don’t want to do the math on your own.
So using this logic, if we calculate our BMR – let’s say it’s 1600 – and we consume less than 1600 calories in a day, we have a caloric deficit. If we’re able to keep this deficit going, we will lose weight. Sounds pretty straightforward…although this isn’t always the case. I can’t even begin to count the number of times I’ve heard “I’ve tried dieting, counting calories, AND exercising, and the weight just doesn’t come off,” or, the even more frustrating statement, “I’ve tried dieting and exercise, and I GAIN weight.” Obviously this is very annoying, not to mention expensive if you’re using any type of subscription weight-loss service. So what do we do next? Well, let’s look at metabolism (and weight gain) from a hormonal perspective, and see how that plays into things.
Metabolism and Hormones
As previously stated, numerous factors influence our metabolism. Hormonally speaking, however, the number of key players are relatively low. Let’s take a quick look at each of them. As a side note, there are many other hormones that influence weight gain, and we’ll get to them a little later.
Insulin: Probably the most important hormone in terms of carbohydrate metabolism, insulin is produced by the pancreas, and affects blood sugar levels. Without getting into too much biochemistry (if you’re in to that, here’s a link), insulin allows glucose (blood sugar) to pass into cells and either be burned for energy, or stored for further use. This is, in essence, a lock and key mechanism. Insulin “unlocks” cells to allow glucose inside, providing those cells with necessary energy. When the cells won’t open for glucose, the glucose is instead stored as fat. This is the main mechanism behind one of the most insidious aspects of weight gain, insulin resistance. Insulin resistance plays a role in multiple conditions, such as diabetes, PCOS, and Metabolic Syndrome, to name a few.
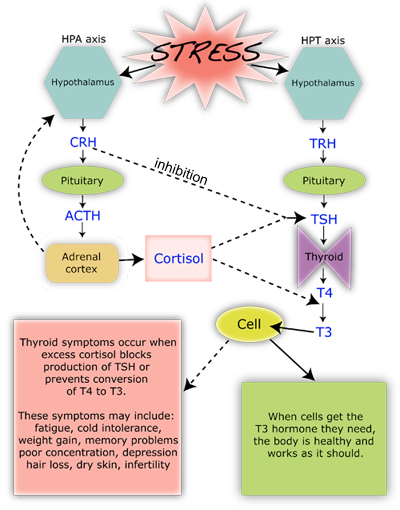
Cortisol: The adrenal glucocorticoid cortisol is the most potent “stress hormone” in our body. It is secreted when our brain perceives we are under stress, be it emotional, physical, or otherwise. Honestly it doesn’t matter if you’re actually under stress or not, if your brain thinks you are, it’s going to tell your adrenal glands to start pumping. From a metabolic standpoint, cortisol activates the sympathetic nervous system (our “fight or flight: response) which causes metabolism to increase, allowing our body to burn through stored energy. In addition, it inhibits the effects of insulin, thereby causing an increase in blood sugar. This is a protective mechanism, as many organs, especially the brain, need glucose to function properly, especially in a high stress situation! Once the stress has resolved, cortisol production decreases, and insulin rises, thereby allowing blood sugar levels to return to normal. In short bursts, this process works wonderfully. With continued, chronic, stress, however (remember, this is perceived stress, too), long-term consequences can arise (see chart below).
Thyroid hormones: The thyroid is in charge of basal metabolic rate. Two main thyroid hormones-thyroxine (T4) and triiodothyronine (T3) are used to increase and decrease metabolic activity as needed throughout the body. T4 is a storage hormone, it is not technically active within cells until an iodine group is removed, and it changes into T3. Let’s look at a diagram…
As you can see above, corticotropin releasing hormone (CRH) blocks TSH production, and excess cortisol effects not only TSH, but the conversion of T4 to T3 as well. In other words, chronic stress affects (via cortisol) thyroid hormone production, and in chronically stressed individuals metabolism is decreased.
So What About Weight Loss?
OK, so we’ve talked a lot about metabolism, and looked at the hormones that affect it. So what about weight? Well, while a higher metabolism can lead to weight loss, just because someone has a higher BMR doesn’t mean that they’ll naturally be thin. Weight loss is a very complicated issue, and as we’ve seen above, metabolism is only a small part of the equation.
I asked my Facebook followers if they had any specific questions about weight loss and hormones, and the response was fantastic. I’d like to answer all of them so for the rest of the blog, so I’m going to do more of a Q&A format. I’ll be including links with these questions, so if you’d like more information on a particular topic, check those sites out!
Q: How do I know my weight issues are hormonal in nature?
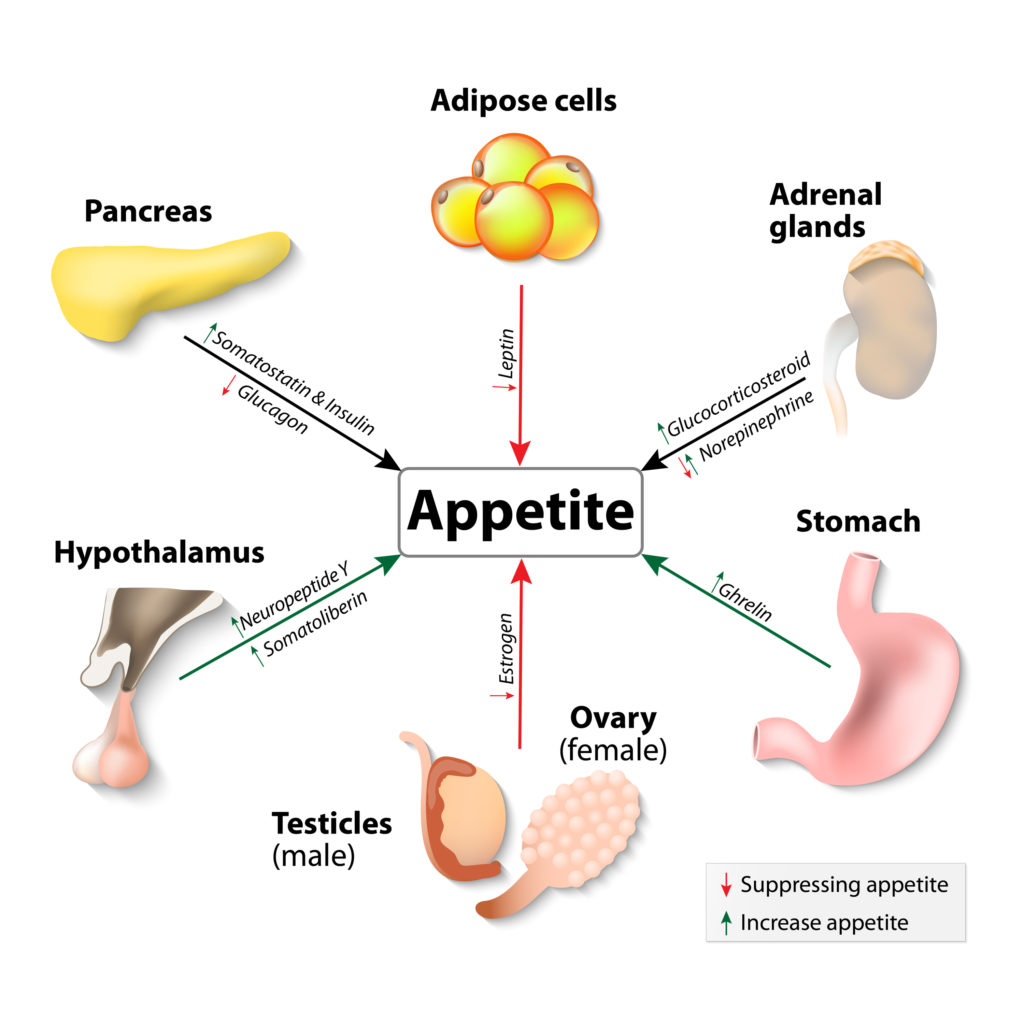
A: The short answer is that weight gain/loss is, by nature, a hormonal effect. Aside from the above listed hormones that effect metabolism, there are a multitude of other hormones that influence how our body stores energy. Let’s look at a few:
Leptin: Leptin is produced in our fat cells (which means it’s affected by insulin), and is considered a “satiety hormone.” When released, it tells your brain that you have enough fat storage, and therefore helps prevent overeating. Interestingly, obese people tend to have a higher circulating amount of leptin in their blood, which points towards leptin resistance as a possible cause of overeating-related obesity. In addition, leptin is reduced with weight loss, which in essence causes your brain to think you’re starving, which is why it’s so hard to keep the weight off after you lose it!
Ghrelin: In contrast to leptin, ghrelin is a “hunger hormone,” and is produced in the stomach. As you might expect, ghrelin levels are highest right before eating, and drop about an hour after you’ve finished munching. In obese individuals, however, research has demonstrated that ghrelin levels may be abnormally low and that they don’t change as much after eating. This abnormal hormonal behavior is thought to be related to elevated circulating insulin levels, which seem to antagonize ghrelin production.
Estrogens: The estrogen family of hormones plays a role in fat storage and deposition. In times of high estrogen production (puberty, early pregnancy) the body shifts fat cells to subcutaneous areas (namely the hips, breasts, and buttocks) and away from deep, visceral (and abdominal) storage. This relocation of adipose tissue is responsible for the “female form,” and explains why women may lose fullness in those areas after they go through menopause. Increased estrogen intake, be it from birth control pills, hormone therapy, or phytoestrogens (flax, soy) may cause the body to go into a fat-storage mode, contributing to weight gain and obesity.
Peptides: Both Neuropeptide Y (NPY) and Glucagon-Like Peptide-1 (GLP-1) affect our desire to eat. NYP is secreted in times of stress, and stimulates our appetite for carbohydrates (which are rapidly converted into blood sugar). Higher protein intake, as well as prebiotic fiber supplementation may be beneficial in reducing NPY release. GLP-1, on the other hand, is produced in our gut when nutrients enter the intestines, and helps regulate fullness. Chronic inflammation has been shown to reduce GLP-1 production, leading to a decreased since of satiety, which may be a reason so many of us eat when we’re stressed!
Q: Why do some women gain weight after a hysterectomy?
A: This is a very common question. First of all, a hysterectomy is a surgical procedure in which the uterus is removed. A complete hysterectomy involves the removal of the uterus and cervix, and a partial hysterectomy is the removal of the uterus alone-the cervix is left intact. From an anatomic standpoint, the uterus does not produce any substantial level of hormone on its own, but rather has a multitude of hormone receptors. Its removal, therefore, shouldn’t cause any substantial hormonal symptom. So what about post-hysterectomy weight gain? While the reasons for undergoing a hysterectomy are many, most women will have a decrease in activity following surgery. This by itself could lead to some short-term weight gain, but once the “all clear” is given to resume normal activities, that weight should come off. What typically causes hormonal symptoms, however, is when the hysterectomy is accompanied by an oophorectomy, or surgical removal of the ovaries. This puts patients into a iatrogenic, or physician induced, menopause. We’ll discuss menopause in detail in a future blog, but the take-home message is that metabolic activity slows after the menopausal transition and estrogen levels decline, causing a shift in fat distribution as stated above. In addition since endogenous testosterone is also decreased after menopause, muscle mass is lost, and the body’s ability to burn fat and excess calories diminishes.
Now I have had patients come in and complain of menopausal symptoms following their hysterectomy, even if the ovaries were left in place. There isn’t really a good medical explanation for this – the research is contradictory. My opinion, however, is when you have multiple patients complaining of the same symptoms following a procedure, there has to be some truth to it. My hypothesis (which is similar to that first study) is as follows: The ovaries received collateral circulation from the vasculature that surrounds the uterus (see picture below). Removal of the uterus can cause a decrease in the blood flow to the ovaries, although not in a substantial enough quantity to cause severe tissue damage. The decrease in blood flow is enough, however, to decrease overall ovarian perfusion, and therefore ovarian function, and decreased ovarian function leads to menopausal symptoms.
Anyone interested in a research study? Let me know!
Q: Can hormones keep me from gaining weight?
A: This is another interesting topic. If you are the type of person that can’t seem to gain weight, no matter what you eat, hormones can definitely play a role. If we rule out obvious hormonal causes such as hyperthyroidism (which boosts metabolic activity), we have to look at those same hunger and fullness hormones listed above. Abnormal levels of Ghrelin and leptin may play a role in people who are chronically thin. Another, albeit not necessarily hormonal cause, would be nutrient malabsorption. Issues with gluten sensitivity, or nutrient and enzymatic deficiency can keep the gut from extracting calories and fats from food, thereby keeping caloric intake low. While this may seem like a “blessing,” nutrient deficiencies and malabsorption actually cause a slew of other symptoms, such as abdominal pain, bloating, as well as diarrhea. If you feel that you are suffering from this condition, I would definitely seek expert care with a gastroenterologist.
Q: Why is a low carb diet good for PCOS?
A: This is an easy one. Many women with polycystic ovarian syndrome also have insulin resistance. In fact, it’s insulin resistance that causes the majority of PCOS symptoms, such as increased facial hair, acne, abnormal bleeding, abdominal weight gain, and oily skin. When insulin levels go up, they suppress Sex Hormone Binding Globulin (SHBG), a regulatory hormone whose sole purpose is to keep free, or unbound, hormones from circulating unchecked. If SHBG is low, then free estradiol and testosterone can run amuck, causing the above stated symptoms. As previously discussed with the insulin paragraph, insulin is responsible for carbohydrate metabolism. Foods that are high in carbohydrates, or more importantly that have a high glycemic index – a measurement of how fast the food is metabolized into glucose – cause a surge in insulin, which over time can lead to insulin resistance. The take-home message for women with PCOS is to try and avoid high glycemic index food. Here’s a list from the American Diabetic Association of foods that have a low glycemic index. We’ll talk more about PCOS in future blogs.
Q: What’s with weight issues and breastfeeding?
A: As to why some women lose weight with breastfeeding, remember that breastfeeding burns an additional 500 or so calories a day. This is because your body is breaking down fat in order to make breastmilk. On the other hand, some women report that they either gain weigh during breastfeeding, or hold onto the weight until they’ve stopped nursing. This is most likely due to either a decrease in activity level, an increase in stress, decrease in sleep, or any combination of the above. In addition, prolactin – the hormone responsible for lactation -causes a down-regulation of estradiol levels. Much like a menopausal woman, a lactating mother will have lower estradiol levels compared to a woman of her same age who is not nursing. This estrogen depletion can cause weight gain as discussed above. I should also state that not eating enough while nursing can lead to weight gain (and a decrease in milk production), as your body goes into “starvation mode,” and holds onto any residual fat stores it has.
Q: Can chronic inflammation lead to weight gain?
A: Of course! Remember cortisol, the body’s most important stress hormone? Well in chronic inflammatory states, our body perceives that inflammation as a stressor, and sends out endogenous corticosteroids to try and reduce it! If you look back up at the graphics, we see that excessive cortisol production not only reduces our ability to utilize insulin effectively, but it also downregulates thyroid function. The end result is more fat deposition, and lowered metabolic activity.
Q: If I’m menopausal (or close to it,) why can’t I lose weight?
A: The menopausal transition brings with it a significant hormonal shift. As a stated above, metabolic activity begins to slow as estrogen and androgen (testosterone) levels naturally decline. A good number of women also report just “feeling worse” during menopause – their sleep quality decreases, they may experience more aches and pains, and they may feel more fatigued, all of which may lower their activity level. This may lead to a multitude of hormonal sequelae, such as:
-Sleep deprivation, which leads to increased stress, which leads to insulin resistance, which leads to weight gain.
-Increased fatigue, which leads to decreased energy, which leads to lowered metabolic activity, which leads to weight gain.
The possibilities go on and on. Keep in mind that as we age our likelihood of developing chronic health conditions rises too, and the diagnosis of something like diabetes mellitus, hypothyroidism, or osteoarthritis can lead to a decrease in activity level as well.
So What Do I Do Now?
Weight loss is a highly controversial, and complex topic, and for me to say something like “let’s just adjust your hormones” downplays how difficult weight loss is. From a medical standpoint, some quicker fixes do exist, such as if someone has insulin resistance, how increasing insulin sensitivity (via diet, medication or supplements) can help shed pounds, or supplementation of thyroid hormone in someone who is hypothyroid. As a general rule though, weight loss is not a simple fix, and in today’s ever increasingly stressful world, it is becoming more difficult to reduce stressors, eat perfectly, and maintain excellent metabolic activity via exercise and supplements.
My advice for those struggling with weight loss is to set realistic goals, and make sure that there isn’t any type of underlying condition hampering your weight loss journey. If you haven’t had a yearly physical, get one – you never know what may turn up. Likewise if there are obvious dietary factors at play (like eating 12 candy bars a day), try and change your diet and see what happens. Additionally, exercise is fantastic, not just for weight loss, but for overall wellbeing and as a stress reliever, and I can’t downplay the importance of a good night sleep, either.
If you’ve done all of those things, and are still struggling with weight loss, you may want to considering seeing a physician who has special training in weight loss therapy. The American Board of Obesity Medicine has a list of physicians who have undergone additional training in the management of weight-related conditions, and is an excellent resource for those patients seeking professional help in their weight-loss journey.
Have you been feeling fatigued lately? Do you feel your sex drive isn’t as high as it used to be? Are you having hot flushes, night sweats, or feeling irritable? Maybe your hair is falling out, or is it growing in places you wish it wasn’t? Well friends, a hormonal issue may be at the root of your problem. In this blog series we’ll look at the hormonal causes of symptoms such as those listed above, and what to do about them. So without further do, let’s get started!
Endocrinology Crash Course
Physiologically speaking, hormones are chemical messengers produced by glands, that fit into specific receptor sites – kind of like a lock and key. When the hormone meets the receptor, a physiologic response takes place. Now keep in mind that these receptors can be all over the body, and that any given hormone can have an effect on multiple types of tissue.
Hormonal symptoms occur when one of the following takes place: the producer gland stops functioning (such as in the case of menopause), there is an excessive amount of hormone produced (what we see in hyperthyroidism), or if the hormone is unable to bind to its receptor (as in the estrogen-blocking effect of Tamoxifen, a medication often used for breast cancer treatment). To complicate things even further, hormone production is regulated by a feedback system – a failsafe, if you will, that attempts to keep too much (or too little) hormone from being produced. If something goes wrong with the feedback system, the downstream effects can be disastrous!
When it comes to treating patients with suspected hormonal disorders, one has to figure out if the issue is with the “producer” or the “target.” Clinical symptoms are often very helpful in determining this differentiation, but as stated above, a singular hormone doesn’t have just one effect. As such, most hormonal evaluations are accompanied by laboratory studies (lots of controversy here). These labs can be performed in a variety different ways, with everything from blood testing, urine testing, or sometimes even salivary or hair follicle testing, to determine the specific value of the hormone at any given time. It is important to note, however, that with a few exceptions these tests provide only a “snapshot in time” of the hormone level in question. As such, a patient may have to undergo multiple laboratory evaluations to get a clear picture of their whole hormonal profile. At this time, serum (blood) testing for sex hormone levels is the recommended method of evaluation and is considered the gold standard by multiple medical specialty societies.
How Hormones are Formed
First things first, that chart above is very intimidating. I remember seeing it for the first time in medical school thinking “holy crap, that’s a bunch of organic chemistry.” I’ve since learned to understand it, but its complexity demonstrates two things:
1: Why endocrinology (hormone disorders) as a specialty exists
2: Why many providers have a difficult time treating hormonal disorders
Now keep in mind that the chart above only shows the sex hormones that are derived from cholesterol. There are literally hundreds of other hormones in the body, but in terms of reproductive functioning, these are the ones that are the most important.
If you look at the color coding on the chart, you will notice some similarities in terms of hormone “families.” Progestogens in yellow, androgens in blue, estrogens in pink, and corticoids in…a color mishmash. The families are based on the number of carbon atoms in the hormone itself, as well as the placement of specific “functional groups,” collections of chemicals that further define the base compound. For example, estrone and estradiol are both made of up 18 carbon atoms (as are all estroGENS), but whereas estraDIOL has two hydroxy groups, estrONE has a ketone group.
I understand this blog is not about organic chemistry, nor would I ever want it to be, so that is about all I am going to say about that.
Hormone Symptom Breakdown
Now that we’ve covered what hormones are, and how they work, let’s look at some hormonal symptoms and potential causes. I’m going to be addressing a good number of these in detail in the upcoming weeks, but for today I thought I would do an overview of many of the hormonal symptoms that I see on a regular basis. As a caveat, the hormones listed below are not the only causes for these symptoms, and as always, this information does not take the place of an actual visit with a licensed provider.
Thoughts: When it comes to weight, you have to look at 2 different things.
1: Metabolism
2: Stress response.
Our metabolism slowly begins to decline once we have 30, due to a very complex assortment of causes, and changes in lifestyle, childbirth, and decreased sleep all can play a role in weight gain. As your thyroid also helps regulate metabolism, a low functioning thyroid can contribute to weight gain, as well. Lastly, stress hormones such as cortisol and insulin, when elevated, decrease your body’s ability to “let go” of fat.
Thoughts: In terms of sexual functioning, testosterone is often the hormone that most people think of. While it is true that low testosterone can cause low sex drive, sexual desire is a very complex subject that is not based on hormonal functioning alone. Sexual pain disorders, especially pain with penetration, can sometimes have a hormonal component. Lastly certain drugs that affect our mood, such as selective serotonin reuptake inhibitors (SSRI’s), can cause a shift in the serotonin/dopamine balance-the neurotransmitters responsible for sexual functioning.
Symptom: Menstrual Mood Disorders
Potential hormonal cause: Changes in estradiol and testosterone
Thoughts: Menstrual-related mood disorders are hormonally due to either a drop in estradiol, or an elevation in testosterone. In the elevated testosterone population, patients often complain of violent, angry outbursts, and in extreme cases, may have had multiple disciplinary actions taken against them at work or school. Conversely, in those with the low estrogen subtype, anxiety, fear, or other avoidance type of activities may predominate.
Thoughts: Elevated androgens – testosterone, dihydrotestosterone, and their precursors (see chart above), are often to blame for unwanted facial and body hair growth, and can cause of a type of hair loss called androgenic alopecia. These symptoms are often found in conditions such as polycystic ovarian syndrome, insulin resistance, and late onset congenital adrenal hyperplasia. Given that the thyroid controls metabolic activity, low thyroid functioning can also result in hair loss.
Well friends, that’s it for the first blog in this series. I hope you enjoyed reading it as much as I enjoyed writing it, and I look forward to delving deeper into different hormonal conditions in the upcoming weeks! As always, if there’s a topic you find interesting, or would like to know more about, let me know!